





抽象的
防止慢性阻塞性肺疾病(AECOPD)的急性加重是一个主要的治疗目标。我们假设,持续增加了呼出一氧化氮的水平(F埃诺)在随访期间,可以识别一组AECOPD风险较高的COPD患者。
为了检验这一假设,我们测量了F埃诺水平(高hysairF埃诺®, Medisoft; Sorinnes, Belgium) prospectively in 226 clinically stable COPD outpatients at recruitment and during follow-up (at 6 and 12 months). Patients were stratified according to the number of visits withF埃诺≥20 ppb.
F埃诺was <20 ppb in all three visits in 44.2% of patients, 29.6% in visit 1 and 26.1% in visit 2 or 3. These three groups suffered progressively higher AECOPD rates during follow-up (0.67, 0.91 and 1.42, respectively, p<0.001). After adjusting for potential confounding variables (log-rank test), the hazard ratio for AECOPD was higher in the latter group (1.579 (95% CI 1.049–2.378), p=0.029). Likewise, time to first moderate and severe AECOPD was shorter in these patients. Finally, there was no relationship betweenF埃诺水平和循环嗜酸性粒细胞。
PersistentF埃诺levels ≥20 ppb in clinically stable COPD outpatients are associated with a significantly higher risk of AECOPD.
抽象的
持续升高F埃诺levels in COPD are associated with a higher risk of exacerbationhttp://ow.ly/fdPy30hdBzo
Introduction
慢性阻塞性肺疾病(COPD)是全球主要的健康问题[1,2]。Acute exacerbations of COPD (AECOPD) represent important events in the course of the disease because they accelerate the decline of lung function [3]并恶化预后[4]和健康状况[5]这些患者。因此,预防AECOPD是COPD的主要治疗目标[6]。
So far, the best predictor of future AECOPD events is past history of AECOPD [7]。More recently,post-hoc大型研究的分析表明,高循环嗜酸性粒细胞计数也与AECOPD频率增加有关[8],重要的是,可以通过吸入的皮质类固醇(IC)来预防和治疗。9,10]这些观察结果可能反映了这些患者气道中的主要T助血2细胞(TH2)炎症反应,因为外周血嗜酸性粒细胞与气道嗜酸性粒细胞相关[11], which, in turn, is a marker of ICS response in COPD [12]。
呼出的一氧化氮馏分(F埃诺)是哮喘中Th2气道炎症的广泛认可和广泛使用的生物标志物[13,14] The role ofF埃诺in COPD is less well established, but it appears to relate to airway eosinophilia [15,16],支气管反应性[17]和对ICS治疗的反应[18]。实际上,F埃诺has been proposed as a potential biomarker of ACO (Asthma–COPD overlap) [19]。在先前的横断面研究中,我们表明,使用十亿分之20(PPB)的截止点,F埃诺可以有效区分不同的COPD表型[20]。然而,纵向再现性F埃诺在COPD及其与COPD结果的潜在关系中(尤其是AECOPD)尚未探索,尚不清楚。我们假设有一组COPD患者F埃诺持续> 20 ppb的水平面临AECOPD的风险增加。我们在一项前瞻性,纵向,观察性研究中检验了这一假设。
方法
研究设计和道德
这项前瞻性的1年随访,观察性研究招募了参加我们门诊三级诊所的患者。患者在招募和6个月和12个月的随访中访问了三次。在随访期间经历过AECOPD的患者被要求将其临床访问延迟至少4周,直到用口服皮质类固醇和/或抗生素完成治疗。
主要结果如下。1)通过可重复性分层的患者分配F埃诺随访期间的测量。就像我们以前的出版物一样[20],根据访问次数将患者分为三组F埃诺≥20 ppb (0, 1 or ≥2 visits). 2) Annualised exacerbation rate and time to first moderate AECOPD (i.e.treatment with oral corticosteroids and/or antibiotics) and/or severe (hospitalisation or emergency room visit for >24 h) [6]。
这项研究是根据1975年赫尔辛基宣布进行的,并获得了我们机构(PEIBA)伦理学委员会的批准。所有参与者都给予了知情同意。
Study population
我们包括当前或前吸烟者的成年人(≥40岁),累积吸烟量≥10岁,并且根据国际诊断标准接受了COPD [6] capable of performing lung function tests serially. Exclusion criteria were as follows: occurrence of AECOPD during the previous 4 weeks, presence of chronic respiratory diseases other than COPD, such as asthma, tuberculosis or α1-antitrypsin deficiency, or current participation in another research study.
Measurements
At recruitment, data on cumulative smoking exposure, previous medical history, concomitant diseases [21],从上一年中,AECOPD的常规治疗以及每个参与者的病历收集。如果在过去3个月内临床稳定性条件下获得了循环嗜酸性粒细胞计数,则记录它们。西班牙版的COPD评估测试(CAT)问卷是自我管理的[22]。临床研究者和患者视而不见F埃诺结果。根据国际建议,测量了肺活量测定法(施用400克沙尔菜醇)[23]。F埃诺以恒定流量测量(50 ml·S−1)与化学发光一氧化氮分析仪(高hypairF埃诺®;比利时米的身),也遵循国际建议[24,25]。
At each follow-up visit (6 and 12 months), patients completed the CAT questionnaire, moderate and severe AECOPD were registered and spirometry andF埃诺确定测量。
Statistical analysis
结果表示为样本量,范围,中值(四分位间范围)或平均值±sd. Categorical variables were compared using the Chi-squared test, whereas continuous variables were compared using ANOVA, the t-test or Mann–Whitney U-test, as required. To account for multiple comparisons, statistical significance was defined as p<0.01. We used Cox regression analysis to compare time to first AECOPD in each group, after adjusting for age, sex, smoking status, previous AECOPD history and ICS use. Analyses was performed using SPSS version 20.0 (IBM corporation, Armonk, NY, USA).
结果
Characterisation of patients
图1presents the consort diagram of the study. We screened 314 patients, of whom 244 were included in the study. 18 were lost to follow-up; therefore, data from 226 patients was analysed.表格1shows their baseline characteristics. Participants were predominantly males of ∼70 years of age, with significant smoking exposure (46 pack-years); approximately 25% of participants were current smokers. Most patients had moderate airflow limitation and the most frequent Global Initiative for Obstructive Lung Disease (GOLD) 2017 groups were B and D. Most patients were treated with long-acting bronchodilators and about half were treated with ICS. The mean exacerbation rate in the previous year was 1.7 events. In 230 (95.5%) patients, circulating eosinophil counts during clinical stability were available; 65% showed eosinophil counts >2%.
Consort diagram of the study.
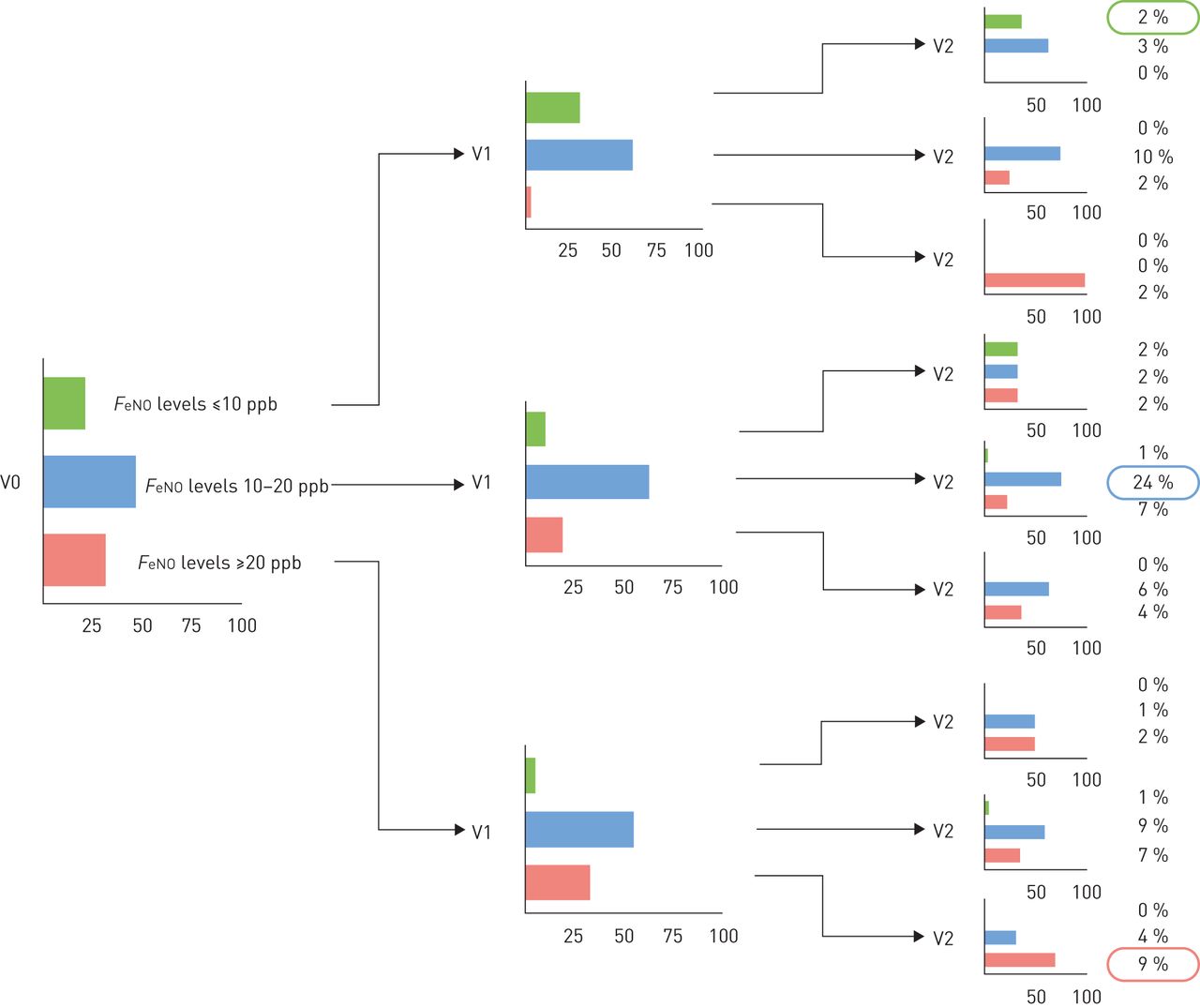
可重复性F埃诺在随访期间
图2presents the reproducibility ofF埃诺随访期间的测量。在基线时,有32%的患者患有F埃诺≥20ppb的水平,46%的水平为10–20 ppb,21%的水平<10 ppb。在随访期间,这些测量值的可重复性为9%F埃诺≥20ppb,10–20 ppb的水平为24%,<10 ppb的水平为2%;因此,F埃诺35%的患者可重现测量。阶层内相关系数(ICC)F埃诺研究期间的测量值较低(ICC 0.387,95%CI 0.234–0.513)。补充图S1显示了平淡的altman图,以比较访问之间的测量值。
呼出的一氧化氮馏分的可重复性(F埃诺) measurement during 12-months follow-up. V0: recruitment; V1: 6 months; V2: 12 months.
表2compares the clinical characteristics of patients withF埃诺levels ≥20 ppb at no visit (n=100) and 1 (n=67) or ≥2 visits (n=59) during follow-up. At baseline,F埃诺在访问次数较大的患者中,较高(p <0.001)F埃诺随访期间≥20ppb。通常,在大多数人口统计学和临床特征中,组之间没有观察到差异,除了反复正常的组外F埃诺levels with a higher female prevalence and less severe airflow limitation. Of note, there were no significant differences in ICS usage, rate of previous exacerbations or circulating eosinophil levels between the three groups (表2)。
随访期间的AECOPD费率和与F埃诺
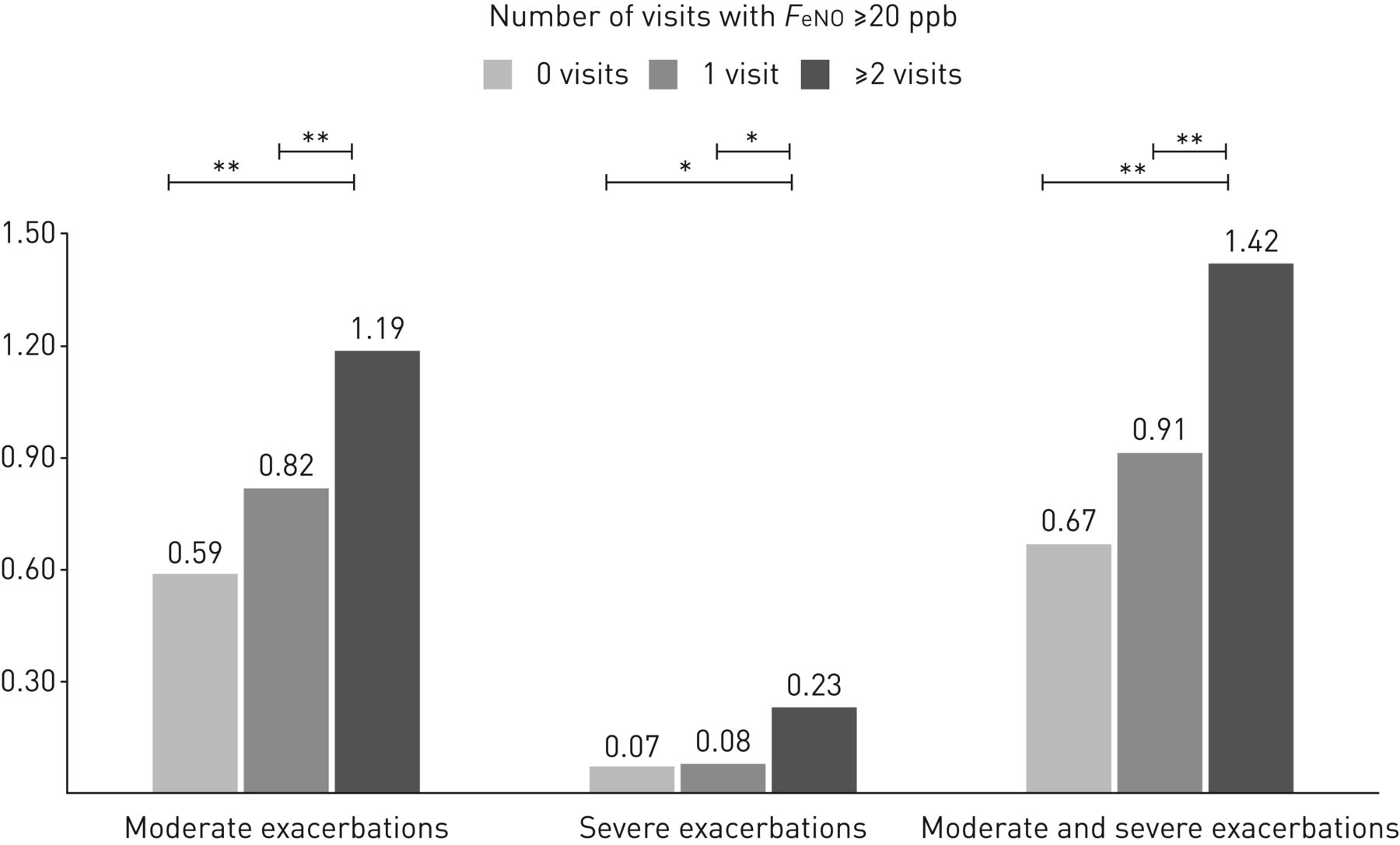
表3compares AECOPD rates and time to first AECOPD by AECOPD severity (moderate, severe and moderate and severe), according to the number of follow-up visits (0, 1 or ≥2) withF埃诺≥20ppb的水平。患者F埃诺≥2次访问期间≥20ppb的中等,重度和中度和重度AECOPD的率明显更高(图3)。≥1个AECOPD患者比例较高的趋势(零访问为46.0%)相对57.1% for one visit相对≥2次访问的61.6%;p = 0.057)和随访期间较高的频繁加重比例(17.0%相对25.7%相对38.5%;观察到p = 0.015)。风险增加主要是由于患者的严重加重驱动F埃诺≥20 ppb during ≥2 visits (表3) after adjusting for confounding variables. Likewise, patients withF埃诺在≥2次研究访问期间≥20ppb显示出第一次AECOPD的时间比其他组短(表3and图4)。
Comparison of acute exacerbation of chronic obstructive pulmonary disease (AECOPD) rate, time to first AECOPD and AECOPD severity levels according to number of follow-up visits with exhaled nitric oxide fraction (F埃诺)水平≥20ppb
研究参与者的慢性阻塞性肺疾病的年度急性加重率,根据呼出的一氧化氮馏分的访问次数分层(F埃诺) levels were ≥20 ppb. *: p<0.05; **: p<0.001.
kaplan – Meier分析时间a)中度和严重,b)中度和c)针对年龄,性别,吸烟,吸入皮质类固醇和先前的病史,对慢性阻塞性肺疾病(AECOPD)的严重急性加重,并根据数量分层呼出一氧化氮部分的随访访问(F埃诺) levels ≥ 20 ppb.
讨论
这项研究表明,患有持续(≥2个随访访问)的COPD患者升高F埃诺值(≥20ppb)具有更高的AECOPD风险,无论先前的ICS使用,吸烟史或先前的AECOPD,尤其是对于需要住院的严重加重而言。因此,监视F埃诺in the clinic can provide useful information to determine the risk of AECOPD in these patients.
以前的studies
本研究中包括的患者的临床特征以及F埃诺此处确定的水平与以前有关的研究相似F埃诺在COPD [18,26]。Likewise, our observation that approximately one-third of the patients showed reproducibleF埃诺levels during follow-up is also in line with previous reports of smaller populations (n=70) [27]。
发现的解释
AECOPD,尤其是那些需要住院的人(i.e.严重的AECOPD)是疾病过程中重要事件,因为它们与肺功能下降,死亡率更高和健康状况较差有关[3–5]。因此,预防AECOPD发作是COPD的主要治疗目标[6]。到目前为止,未来AECOPD的最佳预测指标是以前的AECOPD情节的历史[28]。We hypothesised that persistentF埃诺> 20 ppb的级别与AECOPD的风险增加有关,因为它们是哮喘中Th2炎症的完善的生物标志物,并且众所周知,哮喘 - COPD重叠的患者经常患有AECOPD [29,30]。The results have confirmed this hypothesis because patients withF埃诺≥20 ppb during ≥2 study visits had a significantly higher risk of AECOPD, even after adjusting for other established risk factors, such as current smoking and previous history of AECOPD. Participants with persistently elevatedF埃诺水平显示女性患病率较高,而严重的气流限制与ACO患者先前的报告一致[31]。因此,从本质上讲,我们的结果表明,持续增加的水平F埃诺尽管在本研究中尚未评估这些测量的最佳时机,但在临床实践中可能是ACO的有利生物标志物。
然而,尽管最近观察到表明循环嗜酸性粒细胞计数与AecOPD之间存在关系[32], we found no significant differences in circulating eosinophil counts among groups. Given that the distribution of circulating eosinophils in our study population was similar to that reported in larger populations [8],合理的可能性是嗜酸性粒细胞计数和F埃诺could not predict exacerbations in a similar manner.
Strengths and limitations
我们研究的重要优势包括大型样本量和冗长的随访。但是,有些弱点值得评论。首先,这是一项单中心研究,需要在其他环境中确认结果。其次,我们收集了有关药理学COPD治疗的数据,但在随访期间没有记录这些治疗方法的变化。因此,我们无法分析该潜在混杂因素的影响。最后,该研究的设计在访问期间提供了加重的情况,并且在访问2后没有随访期,因此我们无法评估访问2后发生加重的风险。
结论
这项研究表明,重复出现的COPD患者F埃诺levels ≥20 ppb during follow-up are at an increased risk of AECOPD exacerbations.
补充材料
披露
补充材料
A. AgustiERJ-01457-2017_AGUSTI
B. Alcazar-NavarreteERJ-01457-2017_Alcazar-Navarrete
P.J. Romero-PalaciosERJ-01457-2017_Romero-Palacios
致谢
The authors thank the participants of the study for their willingness to contribute to medical research.
脚注
This article has supplementary material available fromwww.qdcxjkg.com
support statement: This study was supported by Fundacion Neumosur (grant number 01/2011). Funding information for this article has been deposited in theCrossRef资助人注册表.
Conflict of interest: Disclosures can be found alongside this article atwww.qdcxjkg.com
- Received2017年7月19日。
- Accepted2017年10月5日。
- 版权所有©ERS 2018











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}