





Abstract
气流分级新方法的严重限制ation perform better than the percent predicted of the FEV1 and deserve consideration in both prognostic models and individual patient assessmenthttp://ow.ly/oQB030kvVEW
There is broad consensus that airflow limitation, the primary physiological abnormality of chronic obstructive pulmonary disease (COPD), is best defined by a significant reduction in the ratio of forced expiratory volume in 1 s (FEV1) to forced vital capacity (FVC) or to the slow vital capacity. There is also abundant evidence that this reduction is most accurately identified as an individual value less than the lower limit of the normal range (LLN) specific to that individual, as determined from an appropriate healthy, non-smoking, reference population [1]。Because the FEV1/FVC ratio declines normally with age, using a non-individualised cut-off, such as 0.70, has been shown to cause an unacceptable level of misclassification with age and sex bias; this leads to over-diagnosis of 30% or more of older men and under-diagnosis of younger women [2–5]。但是,关于指示疾病严重程度或评估未来结果的可能性的方法的共识要少得多。最常用的索引是FEV的预测值的百分比1, with various cut-off points proposed for categories of severity, and this was endorsed in the 2005 American Thoracic Society (ATS)/European Respiratory Society (ERS) pulmonary function documents [1]。The use of standardised residuals (z-scores) to establish the normal range was recommended by the ERS in 1993 [6] and, more recently, they have also been evaluated as an index of severity [7]。Their use in pulmonary function reporting, particularly as part of a visual scale, has been endorsed in a current ATS technical statement [8]。Both percent of predicted and z-score depend upon the predicted value of FEV1, but predicted values have inherent uncertainty and may not accurately reflect some individuals. Other indices, based upon the absolute value of FEV1, and thus not dependent upon a reference value, have been proposed but are not yet in wide use. Recently in theEuropean Respiratory Journal, Huanget al.[9] reported an evaluation of seven methods to categorise reductions in FEV1,比较的结果的相关性acute exacerbations and mortality. While this study in a Taiwanese population with confirmed COPD was relatively small (n=296) and predominantly male (94%), the results draw attention to some of the less commonly used indices and may cause us to rethink our dependence on percent of predicted.
对于所研究的每种方法,人口分为四个阶段的严重程度,该指数的可靠性通过这些阶层与越来越差的结果的相关性评估。该分析测试了分隔阶段的截止点的索引和适当性。对于五个指数中的每一个,人口都分为四分位数,这具有在阶段之间对称分布的优势,并将差异集中在索引本身上。还通过广泛使用的全球慢性阻塞性肺疾病倡议(GOLD)的临界点评估了预测百分比[10] and the reference-independent index FEV1/height2was also evaluated by previously published cut-off points [11.]。The outcomes studied were frequency of severe acute exacerbations (SAE) at 1 and 2 years and all-cause mortality at a median follow-up of ∼4 years. For each of these outcomes, the reference-based indices (percent predicted both by quartiles and GOLD cut-off points and z-scores) were out-performed by the reference-independent methods. Of these, the FEV1quotient (FEV1Q) performed best. This index, proposed by Millerand Pedersen[12] is simply the absolute value of the FEV1divided by 0.5 for men (or by 0.4 for women) where the denominator represents the first percentile of FEV1values from a large clinical population. As an FEV1Q value approaches 1 it is tracking a patient's course toward the minimum FEV1value compatible with survival (or, at least, with being able to come to a lab and be tested), so it should not be surprising that low values correlate well with mortality. Even though most COPD patients die of comorbidities or during an exacerbation well before reaching this minimal level of lung function, the risk of such an outcome would be expected to increase as this index decreases but, interestingly, the FEV1Q has also been shown to correlate with mortality even in a subpopulation having FEV1within the normal range [12]。The study by Huanget al.[9]确认M的发现illerand Pedersen[12] that the FEV1Q correlated better with mortality than two other reference-independent indices proposed earlier, FEV1/height2and FEV1/height3,除了表明FEV外1与这三个相互关联的SAE outc问相关omes. The percent of predicted by quartiles also correlated well with mortality, but not with SAEs, while percent predicted by GOLD correlated less well with both, and z-scores showed a good correlation only to an adjusted model for mortality. Most of the indices showed an inversion with a higher likelihood of mortality or SAE or both in the third quartile than in the fourth (lowest) quartile. This may reflect an anomaly in this relatively small population, but this inversion of quartiles was not seen for FEV1Q在研究的四个结果中的任何一个中。
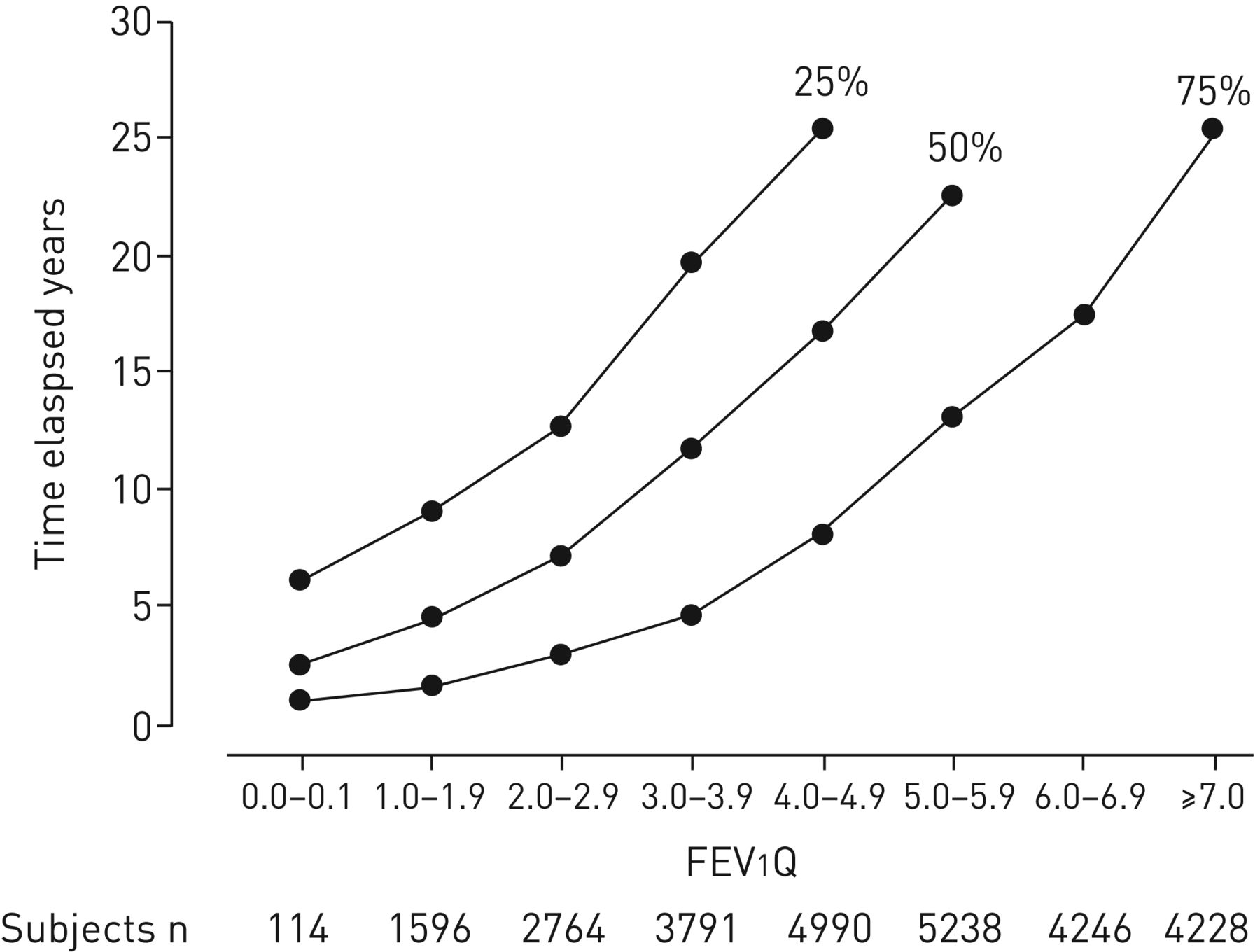
Epidemiological studies can use an index of severity as a continuous variable or with population specific cut-off points, but clinical use has typically placed deficits in staging categories such as mild, moderate and severe, which require predetermined cut-off points. While the analysis by quartiles has the advantage for this study of allowing like−like comparisons between the methods, the cut-off points that result may not translate to other populations, but do inform the choice of more generic cut-offs. For example, in the clinical COPD population reported by Huanget al.[9], the quartile breaks for FEV1percent predicted occurred at 69, 53 and 41%, while the GOLD divisions at 80, 50, and 30% placed 81% of the patients in the two mid-levels with only 12% in the highest and 7% in the lowest. Note that because this study defined obstruction by the Global Lung Function 2012 Initiative LLN for FEV1/fvc [13.], rather than 0.70, the false-positives usually seen by GOLD would not be included. For FEV1Q the quartile cut-off points in the clinical population of the current study were 3.4, 2.5 and 1.9. The study by Millerand Pedersen[12]结合了大型肺功能实验室(n = 11 972),一般人群(13 900)和临床COPD人群(1095)的数据集。在这种成年人口混合的结果中的结果分布(figure 1)表明有6%的人有FEV1Q <2 with median survival of <5 years, 24% had an FEV1Q为2–4,中位生存率约为10年,有38%的FEV1Q of 4–6 with median survival of about 20 years, and 31% had an FEV1Q> 6,有75%的生存超过20年。在其他临床人群研究之前,这些数据表明6、4和2的整数值将使死亡率风险方便。
![The 75th, 50th and 25th percentiles of survival in years for each unit of better lung function as measured by the forced expiratory volume in 1 s quotient (FEV1Q) index. The distribution of subjects in a mixed general and clinical population is shown below the graph. Reproduced with permission [12].](http://www.qdcxjkg.com/content/erj/52/2/1801005/F1.large.jpg?width=800&height=600&carousel=1){kind=link}
{kind=link}
The 75th, 50th and 25th percentiles of survival in years for each unit of better lung function as measured by the forced expiratory volume in 1 s quotient (FEV1Q) index. The distribution of subjects in a mixed general and clinical population is shown below the graph. Reproduced with permission [12]。
The various expressions of FEV1有不同的效用,可以是互补的。个人测试的放置在与正常人群的关系中,i.e。确定结果是异常的可能性,最好是由Z分数完成,其中LLN为-1.645,相当于健康参考人群的第五百分点。但是Z分数和百分位数都有局限性作为严重性指数。对于z得分,所有个体的测量单位(正常人口的标准化残差)都是相同的,因此,任何负z得分代表年龄较小的个体比年轻,更高的个体的比例减少。当以健康人群的百分位数表示时,所有异常FEV1values are clustered below the fifth percentile with 40–50% of COPD patients falling below the 0.5th [7]。The percent of predicted is not well suited for diagnosing abnormality because the value representing the population LLN varies with the individual and with the test; however, it does provide an intuitive estimate of any decrement in lung function and is easily understood by patients. While percent of predicted shows the loss from a predicted normal value, FEV1Q shows how much function is left before reaching a minimal value, so it may be most helpful to clinicians in evaluating the later stages of disease. Because FEV1Q is independent of a reference source it may be particularly helpful in older individuals where there is more uncertainty in the predicted values. This has been demonstrated at age ≥65 years by a better correlation with mortality for FEV1Q比具有COPD的组和一个没有气流限制的组所预测的百分比[14], and in a population-based sample age ≥80 years for mortality and other adverse outcomes [15.]。
Indices based upon the FEV1are the most commonly used measures of lung function in staging or prognosis of COPD and other obstructive diseases, but others may also have a role. The FEV1itself, expressed by absolute value, has been shown to correlate better with exertional dyspnoea than when “corrected” for sex, size and age by percent of predicted [16.]。FVC has been shown to correlate better than FEV1with all-cause mortality in general populations [17.], most likely reflecting the large role of cardiovascular and other diseases as causes of death. While the large population variability of the forced expiratory flow at 25–75% of FVC (FEF25–75) has made it unhelpful for the diagnosis of airflow obstruction [18], there is interest in trending its change, or that of the ratio of FEF25–75/FVC, in individual patients at risk for transplant-related obliterative bronchiolitis or early in the course of cystic fibrosis [19.,20.]。Efforts to improve clinical staging or predict future outcomes will add other risk factors, such as age and smoking history, to an index of lung function. A GOLD update added history of exacerbations and symptoms to the FEV1百分比预测上述截止点,但这并不能提高其预后有效性[10,21.] The BODE index added body mass index, a dyspnoea score and walking distance [22.]。Other candidates include frailty [23.], phenotypes [24.,25.] and biomarkers [26.,27]。These more complex prognostic models may be improved by including FEV1Q, and are a valuable research tool, but the clinician dealing with an individual patient needs a simple, easily calculated guide to severity. The demonstrated value of the FEV1Q as a predictor of clinically important outcomes in population research suggests that it deserves attention for individual patient assessment as well.
Footnotes
Conflict of interest: None declared.
- ReceivedMay 30, 2018.
- AcceptedJune 13, 2018.
- Copyright ©ERS 2018
References










