





一个bstract
this study aimed to estimate time trends in the lifetime risk of hospitalisation with exacerbation of chronic obstructive pulmonary disease (COPD) in Denmark.
during the period from 1994 to 2008, a register-based cohort study was conducted covering each subject in the entire population of Denmark (5.18 million in 2008). Based on previously validated diagnosis codes, all COPD hospitalisations were identified. Individual retrospective review periods of 8 years were used to determine first-time hospitalisations. From year 2002 to 2008, all first-time COPD hospitalised subjects aged ≥30 years were identified. The calculation of lifetime risk was based on age- and sex-specific first-time COPD hospitalisation rates and rates of COPD hospitalisation-free survival, assuming them to be calendar time stationary.
the study included 23.9 million person-years of risk time and identified 48 959 first-time COPD hospitalisations. For 30-year-olds in Denmark, the lifetime risk of COPD hospitalisation was 12.0% (95% CI 11.9–12.2) for females and 10.9% (95% CI 10.8–11.1) for males. Trends were generally equal in both sexes.
在2002年至2008年期间,首次COPD住院率下降,而从未COPD住院受试者的生存率增加。我n consequence, the lifetime risk of COPD hospitalisation remained constant.
一个bstract
COPD住院的10%终身风险保持不变http://ow.ly/mxsU0
我ntroduction
Chronic obstructive pulmonary disease (COPD) is a preventable disease, but the exposure to inhaled gases and particles,例如。tobacco smoke, which is the major cause of the disease, usually begins decades before symptomatic disease can be detected [1]。由于因果关系的暂时分离,并且并非所有吸烟者都活着发展这种疾病,因此发展疾病的风险估计对于个人的预防咨询很重要。此外,对于医疗保健计划者,需要估算风险估计来预测其未来负担,并优先考虑COPD和其他可预防的健康风险之间的预防资源。
risk is preferably estimated as the age-specific incidence rates. However, the full spectrum of age-specific incidence rates is difficult to communicate to patients and politicians, and also to compare across countries and diseases. Furthermore, the risk of developing a chronic disease, such as COPD, at some future age (the age-specific incidence rate) provides little information to a patient, if the chances of surviving until that age without already having developed the disease are not considered.
终生风险估计值通过总结年龄特异性发病率的频谱和无病生存率的频谱来克服这一问题[2,,,,3]。此类估计是关于其他慢性疾病(例如心血管疾病和癌症)通常使用的基准,但直到最近才在COPD中采用[4,,,,5]。
以前的少数COPD终身风险研究[6-8]并没有集中于发展COPD终点的风险,在这种风险中,死亡率,降低质量和医疗保健成本最高,并且疾病加剧的住院治疗经常[9-12]。
这项研究旨在估计丹麦COPD住院终生风险的时间趋势。
methods
设计
during the period from January 1, 1994 to December 31, 2008, a register-based cohort study was conducted covering each subject in the entire population of Denmark (5.18 million in 2008 [13])。
data sources
我n Denmark, healthcare services are in general free of charge and with equal access for all citizens. COPD hospitalisations are to public hospitals and occur either by referral from a general practitioner or, in severe cases, as direct emergency admissions.
since 1977, the Danish National Patient Registry has recorded administrative data from all Danish admissions to hospital [14]。从1994年及以后,根据国际疾病分类第10修订(ICD-10)进行诊断[ICD-10)[15]。一个ll data are registered with the patient's unique civil registration number, which allows data linkage on an individual level between all national registers [16]。
在1994年至2008年期间,我们确定了丹麦COPD的所有住院治疗,并将个人卫生行政数据与来自人口统计学登记册的数据联系起来,涉及患者的出生,死亡和迁移或丹麦的迁移。在2002年至2008年期间,人口统计学登记册还提供了丹麦总人口的年龄和性别特定的受试者和死亡人数。
definition of hospitalisation with COPD
COPD住院定义为ICD-10代码J41-44(COPD,慢性支气管炎或肺气肿)的任何住院继发诊断。
除包括J41-43的包含外,丹麦医疗保健系统中使用上述诊断代码的组合来监控和支付COPD的医院治疗,并且2008年全国验证研究发现J44作为主要的预测价值为93%,主要预测价值诊断为呼吸衰竭或肺炎的继发于87%[14]。the inclusion of J41–43 (chronic bronchitis and emphysema) was suggested in the validation paper to obtain the best possible sensitivity and specificity. In a prior study, we showed that hospitalisations coded with J41–43 did not significantly differ from those coded with J44 (COPD) [17]。敏感性分析遗漏了肺炎作为主要诊断,仅包括J44作为主要诊断。
definition of incident and prevalent cases
首次COPD住院(事件案件)被定义为在有关住院治疗前的8年内未在8年内住院的受试者的任何COPD住院。相应地,受试者被归类为第一次COPD住院和死亡,迁移或8年的个人随访期结束,没有COPD住院治疗(以先到者为准)。选择了7年的研究期和较长的8年回顾性审查期,因为ICD-10分类数据仅在1994年至2008年才能获得,我们希望既无偏趋势估计,又避免被认为是同一受试者的可能性在我们的学习期间,初次住院了两次。对回顾性审查期的长度进行了敏感性分析,将其在总体估计中降低到5年,并将其增加到14年,仅在2008年才有可能。
estimation of lifetime risk
每年1月1日从2002年到2008年,所有达尼sh subjects aged ≥30 years were categorised as being either prevalent or at risk of first-time COPD hospitalisation. For each calendar year, all subjects at risk in the beginning of the year were further categorised as having either died or been hospitalised with COPD (whichever occurred first), or as remaining at risk throughout the year. Using 1-year age strata from age 30 years until >99 years, the age- and sex-specific number of subjects in each category was calculated for each calendar year. The incidence rates of first-time COPD hospitalisations and the mortality rates of subjects never hospitalised with COPD were estimated from the number of incident subjects and the number of subjects who died before COPD hospitalisation, respectively, divided by the number of subjects at risk in the beginning of each year.
计算年终身风险估计的关键是,假设在未来的寿命中,从30岁到99岁以上,上述年龄特异性发病率和死亡率将保持恒定。有了这个假设,k描述的方法eiding[[2]用于估计COPD住院的终身风险。
For each age from 30 years to >99 years, the probability of COPD hospitalisation-free survival from age 30 years until a given age was calculated as the product of the age-specific probabilities from age 30 years until that given age. The conditional probability of being hospitalised with COPD at a specific age, given COPD hospitalisation-free survival from age 30 years until that given age, was calculated as the product of the age-specific COPD-hospitalisation-free survival probability and the incidence rate of first-time COPD hospitalisation at the given age. Finally, the residual lifetime risk at a given age was calculated as the sum of the above conditional probabilities from that age until age >99 years. Confidence intervals were calculated using bootstrap techniques. All analyses were performed using STATA Release 11.0 (STATACorp, College Station, TX, USA).
我们在30岁时开始计算,因为诊断代码从该年龄开始得到验证,并且因为该年龄之前的COPD住院非常罕见。因此,我们在登记册中确定的少数年轻人可能患有哮喘,就像更频繁的0-2岁儿童也与COPD编码的儿童很可能已经完全不同。
该研究得到了丹麦数据保护局(参考号2009-41-3337)的批准。根据丹麦立法,该研究是基于登记册的,因此不需要生物医学研究伦理委员会的批准。
results
在2002年至2008年期间,年龄≥30岁的丹麦人口从3.39人增加到351万人,而观察到的累积人口COPD住院时间为2390万年。我们确定了22个749名男性,首次接受COPD住院和2610名女性。先前的论文中表征了≥45岁(97.5%)的患者的住院治疗;住院死亡率从5.9%增加到7.0%和1年的死亡率从23.2增加到25.9%[17]。
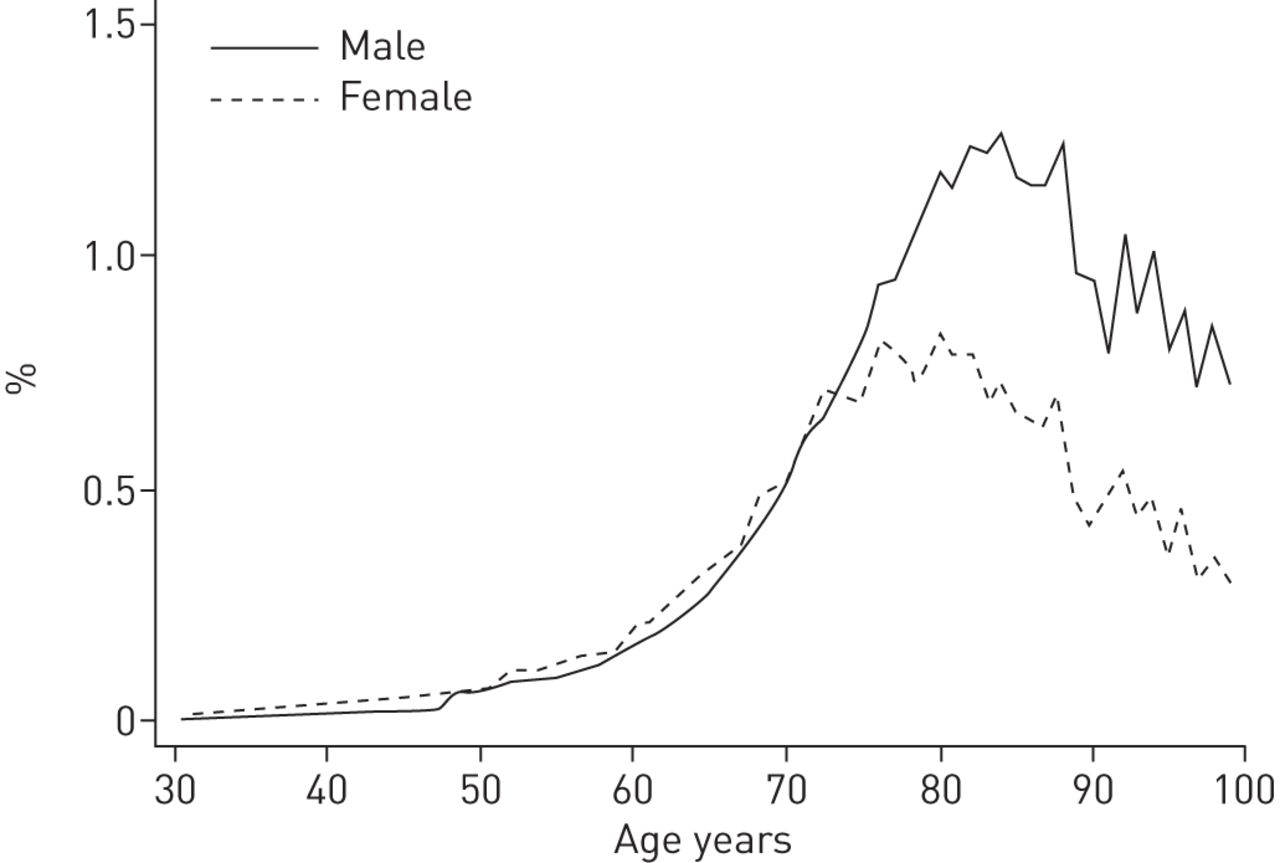
在≥30岁的丹麦人中,女性的首次COPD住院发病率为每1000年2.14年(95%CI 2.11-2.16),男性为1.95(95%CI 1.93–1.98)((95%)(95%)((table 1)。the risk of first-time COPD hospitalisation increased with age until ∼80 years for females and 85 years for males. Above these ages, the risk decreased with increasing age (如图。1andtable 1)。
1年内首次慢性阻塞性肺部疾病住院的风险。
从2002年到2008年期间,在两种sexes, the residual lifetime risk for 30-year-olds to be hospitalised with COPD remained roughly constant. Therefore, no further trend analyses were made. Based on the total period, using the main case definition, the risk was 12.0% (95% CI 11.9–12.2) for females and 10.9% (95% CI 10.8–11.1) for males. Using the strictest case definition, exclusively J44 as primary diagnosis, the risk was reduced to 9.6% in females and 8.4% in males (table 2)。
30岁儿童的剩余寿命风险主要包括45至90岁之间的条件概率(如图。2)。这是由于首次住院和无住院生存率的低点低于此年龄间隔和以下。
一个ccumulated incidence of first-time chronic obstructive pulmonary disease hospitalisation for 30-year-olds, adjusted for the competing risk of death.
从30岁开始,对于女性,残留寿命的风险随着年龄的增长而不断降低。对于男性,剩余的寿命风险略有增加,直到48岁,之后减少。直到65岁时,女性的风险较高,但高于该年龄,男性风险较高(如图。3andtable 3)。
慢性阻塞性肺部疾病住院的残留寿命风险。
将2008年分析的回顾性审查期从8至14岁延长并不能大大降低终身风险估计,同时将回顾性审查期降低到整体分析中的5年,使男性的终身风险估计从10.9%提高(95(95)%CI 10.8 - 11.1)至11.6%(95%CI 11.4 - 11.7),女性为12.0%(95%CI 11.9 - 12.2)至12.8%(95%CI 12.7 - 13.0)。
讨论
this is the first study to estimate the lifetime risk of COPD hospitalisation. Data from 15 years of continuous and complete coverage of all 5.43 million citizens of Denmark were analysed and the main observation is that, for 30-year-old Danes, the lifetime risk of having a COPD exacerbation requiring hospitalisation is 12% for females and 11% for males. Considering the 25% 1-year mortality and the fact that multiple minor to moderate exacerbations as well as many years of progressive symptoms and reduced quality of life usually precedes hospitalisation with COPD [12,,,,18], this study confirms that COPD is among the most important public health problems.
三项先前的COPD研究报告了普通人群的终身风险。在加拿大安大略省,使用来自初级和二级护理的价值14年的约600万受试者的经过验证的寄存器数据,GErshon等。[[6]报告说,女性有26%的女性和30%的男性患医生诊断的COPD的风险。在一项类似的荷兰研究中,包括约18.5万受试者在全国各地的400种常规惯例中fonso等。[[8] reported a substantially lower 8.3% female and 12.7% male risk. In that study, however, all records of potential COPD underwent expert review using a somewhat stricter case definition. In contrast to the register-based studies of physician-diagnosed COPD,vandurme等。[[7]进行了11年的队列研究。同样在荷兰,每2 - 3年进行了每2至3年的肺活量测定法,在医院和初级保健以及通过药房记录中进行额外随访。该研究报告说,女性有16%和24%的男性患COPD的风险。
尽管上述研究与我们的研究不同,但恒定的未来年龄特异性率的假设和计算终身风险的基本原理都是相似的。但是,由于致命合并症的高频率和疾病的缓慢进展,许多患有COPD早期阶段的患者将死于其他原因,然后再住院COPD。另外,一些患者会出现致命的COPD,尽管他们从未住院过这种疾病。因此,与本研究中发现的风险相比,上述风险更高,仅仅是因为患者在疾病的早期阶段被诊断出来。G的研究分别通过较低的死亡率为5%和6%。Ershon等。[[6] and Afonso等。[[8], respectively. Other major differences from our study include the fact that the studies by GErshon等。[[6] and Afonso等。[[8]排除80岁以后的COPD首次亮相,这种方法将使我们的估计值降低约25%(如图。2)。一个lso, the two latter studies used variable retrospective review periods of at least 1 year and at least 5 years, respectively. Reducing the retrospective review period would increase our lifetime risk estimate as demonstrated. Making it variable,例如。从2002年的8年到2008年的14年,将略微降低风险估计,但会引起时间趋势的偏见。最后,GErshon等。[[6] andvandurme等。[[7] estimates are dated nearly one decade prior to ours and both the COPD incidence rates and mean life expectancies on which they are based probably have changed since then.
优势和局限性
the major strengths of this study include the size and duration of the study, the complete coverage of an entire nation, and the exact dates of hospitalisations, births and deaths. Also the homogenous equal access free-of-charge Danish Healthcare system supports equality in the decision criteria to hospitalise across the population.
测试了从注册表中获得的COPD诊断高度有效[14]。然而,错误分类仍然是我们研究的潜在局限性,并且没有肺活量测定数据可以进一步验证诊断。因此,我们的研究包括一些住院,患者被错误诊断为COPD。但是,它可能也未能包括更多由COPD引起的住院治疗,但对其他诊断进行了错误编码[14]。
在涵盖一般人群的大型登记册中,不存在有关解释因素的数据,例如吸烟状况和肺活量测定法。此外,关于终身风险的任何结论例如。吸烟,将要求所有研究的受试者在整个研究期间保持相同的吸烟状况,并且可以合理地假定保持这种确切的状态,直到死亡或研究的事件发生。因此,无论研究方法如何,除了性别之外,这些要求几乎总是无法满足这些要求。
the lifetime risk of COPD hospitalisation varies among populations because of different incidences of severe COPD exacerbations, different thresholds for admission to hospital, and different life expectancies. For decades the proportion of daily smokers has been higher in Denmark relative to other developed countries, especially among females [19]。Furthermore, the rate of COPD hospitalisations in Denmark [17] is somewhat higher than in contemporary studies from the USA [20-22],挪威,瑞典[23] and France [24]。因此,与其他发达国家相比,丹麦的COPD住院终身风险可能更高。但是,丹麦的平均预期寿命与美国相同,但比大多数欧洲国家短[19]。较短的平均寿命意味着所有疾病的寿命降低,主要发生在老年时。因此,在其他国家,通常比丹麦更健康的COPD住院风险更高。住院严重程度阈值可能在国家之间有所不同。但是,丹麦COPD住院的特征与其他发达国家一致。例如,丹麦,美国和英国的住院死亡率,年龄,性别和住院时间相似[9,,,,17,,,,25]。
the main limitation of any lifetime risk study lies in the necessary assumption of time homogeneity of incidence and mortality rates [2,,,,3]。Continuation of the increase in mean life expectancy, which has been steady for more than two centuries [19,,,,26], will increase the lifetime risk of COPD hospitalisation. Meanwhile, improved treatment possibilities and reductions in harmful airway exposure will decrease it.
我n Denmark, during our observation period, the total number of COPD hospitalisations as well as the age- and sex-adjusted incidence rate of first-time cases decreased ∼8% [17]。在同一时期,住院费的发病率和患病率在年龄段> 80岁的年龄段中增加了约20%,而下面的年龄组则下降了约20%。这些大的双向年龄特异性趋势已被解释为是由于1920年左右出生的出生队列的老龄化所致,它们更容易受到两种香烟的烟雾[27]和职业尘埃比出生之前和之后出生[28]。此外,1920年之前出生的出生队列的暴露率低解释了这项研究的观察结果[8] that, in the oldest age group, COPD incidence actually decreases with increasing age. Furthermore, during our study period the ratio of patients treated with inhaled corticosteroids and tiotropium prior to their first COPD hospitalisation improved substantially [17]。这可能对COPD住院率产生了降低的影响。
during our study period, there were some considerable changes in the Danish healthcare system. A 12% reduction in the number of hospital beds for COPD patients and at the same time fewer hospitalisations and increased inpatient mortality lead to the conclusion that the severity threshold for hospitalisation with COPD increased [17]。
during the period from 2002 to 2008, in both sexes, the concurrent underlying mixture of increasing Danish overall life expectancy [19]并降低了首次COPD住院的发病率使COPD住院的终生风险不断。这种平衡不太可能保持稳定。但是,未知的是,预期寿命的增加或COPD发病率是否会更强。
平均预期寿命和寿命风险的估计是基于相似的假设,因此具有相似的特征。在大多数人群中,已知的出生队列效应使平均预期寿命成为对新生儿寿命的估计。同样,我们研究的基本变化使得对30岁的年轻人的估计值比80岁的年龄较小。但是,在人群中,平均预期寿命被认为是一般健康的有效指标,同样,疾病的生命风险可能是其负担最强,最强大的指标。
Conclusion
根据目前的住院和存活率,在所有30岁丹麦人的寿命中,将在COPD住院。两性的趋势通常相等。在2002年至2008年期间,首次COPD住院率下降,而从未COPD住院受试者的生存率增加。结果,COPD住院的终身风险仍然是恒定的。
一个cknowledgments
We wish to thank secretary Lise Keller Stark (Research Unit of General Practice, Institute of Public Health, University of Southern Denmark, Odense, Denmark) for proofreading the manuscript.
Footnotes
支持声明:这项研究得到了来自Jesper Lykkegaard的研究奖学金的支持南丹麦大学,以及来自Governmental Region of Southern Denmark。
Conflict of interest: Disclosures can be found alongside the online version of this article atwww.www.qdcxjkg.com
- received2012年8月17日。
- 公认january 22, 2013.
- ©ERS 2013











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}