





向编辑:
肺水肿中的肺水肿通常可归因于充血性心力衰竭或静脉闭塞性疾病。在这里,我们报告了一种罕见的肺水肿,这是由于抗纤维型纵隔炎的肺静脉狭窄。
Our patient was a 44-yr-old female who was admitted to our hospital because of acute dyspnoea. She had a histogically confirmed cutaneous sarcoidosis diagnosed 17 yrs prior to presentation at our hospital and had received aminoquinolins for 9 yrs. 1-yr prior to presentation at our institute, pulmonary involvement was diagnosed based on clinical complaints (progressive dyspnoea and non-productive cough) and diffuse pulmonary infiltration with bilateral hilar enlargement on chest radiography. On admission to our hospital, the patient was orthopnoeic and polypnoeic, and had dilatation of jugular veins suggesting congestive cardiac failure. Arterial blood gases in room air showed hypoxaemia (an arterial oxygen tension level of 62 mmHg) and hypocapnia (a carbon dioxide arterial tension of 30 mmHg). Transthoracic echocardiography showed right ventricular dilatation and high systolic pulmonary artery pressure at 45 mmHg, while the left ventricular function appeared normal. Pulmonary ventilation–perfusion scintigraphy showed mismatched perfusion defects in the upper left lobe and matched ventilation–perfusion defects in the right lung. Contrast-enhanced computed tomography (CT) (fig. 1⇓)显示:软组织衰减纵隔肿块,具有钙的焦点;不同程度的左上方和右下肺静脉,左上方的总闭塞近,左上方近肺静脉,没有任何阻塞肺动脉;实质和胸膜迹象,所有典型的静水压肺水肿(地面玻璃衰减,阴道隔膜增厚和双侧胸腔积液)(图1A⇓and b); and absence of thrombosis of pulmonary arteries. Pulmonary function showed a total lung capacity of 74% predicted, a vital capacity of 70% pred, forced expiratory volume in 1 s of 65% pred and a transfer factor of the lung for carbon monoxide of 57% pred. Sarcoidosis fibrosing mediastinitis complicated by pulmonary oedema and pleural effusion due to pulmonary venous obstruction was diagnosed. Diuretics, anticoagulant therapy and oxygen were initiated, followed by steroid therapy (prednisone 1 mg·kg−1·d−1). Under treatment, a dramatic and rapid improvement of dyspnoea and a normalisation of haematosis were observed. After 1 month of treatment, a new CT scan showed regression of pleural effusion and lung ground-glass attenuation, while all other abnormalities, particularly in the mediastinum and concerning pulmonary veins, remained unchanged. The treatment was continued for 1 yr while tapering steroid therapy. Transthoracic echocardiography showed pulmonary hypertension with a systolic pulmonary artery pressure of 40 mmHg and a normalisation of right ventricular volume. 1 yr later, pulmonary function remained unchanged, while a thoracic CT scan showed a slightly reduced soft-tissue attenuation mediastinal mass with an increased number of calcifications (fig. 2⇓) and no sign of pulmonary oedema or pleural effusion. Conversely, there was no change in the pulmonary vein stenosis.
{kind=link}
{kind=link}
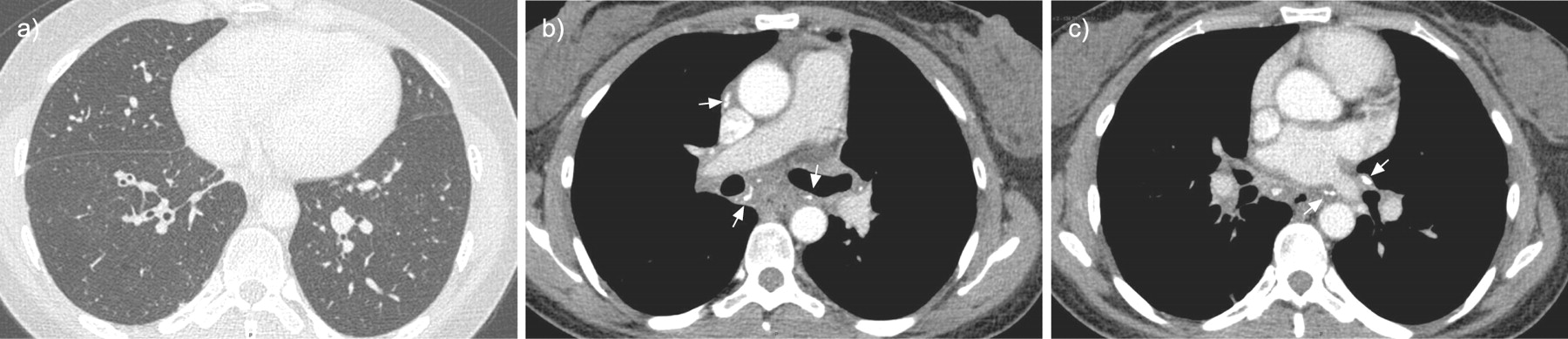
Contrast-enhanced computed tomography at admission showing signs of a and b) parenchymal and pleural signs of hydrostatic pulmonary oedema (lung window settings image), including central ground-glass attenuation, bilateral pleural effusion and thickening of interlobular septa in the upper lobes. c and d) A soft-tissue attenuation mass (star) with foci of calcifications (white arrow) was noted (mediastinal window settings image) without contrast enhancement of the left superior (c) and right inferior pulmonary veins and stenoses of the left inferior pulmonary vein (black arrow) (d).
{kind=link}

{kind=link}
Contrast-enhanced computed tomography 1 yr later showing a) no sign of pulmonary oedema (lung window settings image) and b and c) slightly reduced soft-tissue attenuation mediastinal mass with increased number of calcifications (white arrow) (mediastinal window settings image) while pulmonary vein abnormalities remained unchanged.
据我们所知,我们在本文中报告了第一种患有纤维化含有含有氨基炎诱导的肺静脉梗阻的肺水肿诱导的肺静脉梗阻。CT成像证明肺水肿的诊断支持,纤溶纵隔炎和肺静脉狭窄。可以根据超声心动图撤回充血性心力衰竭,尽管搅拌闪烁的通风灌注失配,但肺栓塞被排除。有趣的是,这种机制将被添加到静脉闭塞性疾病中,作为肺水肿中的肺部水肿的非心脏病。
纤维化的纵隔炎最常见是由于结节病的原因1: infectious diseases (histoplasmosis, tuberculosis, aspergillosis, blastomycosis and cryptococcosis), autoimmune disease, Behçet’s disease, radiation therapy, Hodgkin’s disease and idiopathic. Regarding sarcoidosis, Devarajet al.2reported two cases in a series of 12 patients, with CT images and histology of fibrosing mediastinitis (16.6% of patients). Vascular obstruction due to fibrosing mediastinitis is frequent3–13, particularly during histoplasmosis. Superior vena cava obstruction is the most commonly reported and is easily diagnosed. Pulmonary artery obstruction has also been reported3–6。In sarcoidosis, two cases were reported by Hamilton-Craiget al.7who were successfully treated by stent placement in the pulmonary arteries. Conversely, there are only a few cases in the literature of pulmonary venous obstruction10–13。This happened in three of 64 patients (4.6%) with fibrosing mediastinitis in the study by Schowengerdtet al.11。Clinical manifestations include cough, progressive respiratory distress and haemoptysis. This pattern of symptoms has been called the “the pseudo-mitral stenosis syndrome”1。肺部静脉阻塞逐渐发生,因此症状可能会延迟,诊断难以捉摸。在疾病的晚期阶段,具有多于一种肺静脉闭塞,可能发生肺水肿的反复发作,并且通常是死亡的原因12–14。
There is no well-established treatment for fibrosing mediastinitis. With regard to the present case, we hypothesise that the rapid improvement after treatment was mainly attributable to diuretics. Conversely, steroids had little or no beneficial effect as pulmonary hypertension and pulmonary vein obstruction remained unchanged. Such absence of response to steroids has previously been reported in a case of pulmonary arterial stenosis secondary to sarcoidosis mediastinitis15。
In conclusion, clinicians must be aware of this possible cause of acute respiratory insufficiency in sarcoidosis in which both thoracic CT and echocardiography appear crucial for establishing the diagnosis. In such a case, symptomatic treatment is mandatory but steroid therapy may be poorly efficient when fibrotic lesions in the mediastinum make up the main mechanism of pulmonary vein stenosis.
Statement of interest
没有宣布。
- ©ers Journals Ltd
参考资料










