





一种bstract
These large-scale studies confirm previous findings about a slightly increased incidence of COVID-19, but not of severe COVID-19, in asthma patients. Still, no definitive conclusions can be drawn since many bias factors have not been taken into account.
Text
2019年的冠状病毒病(COVID-19)大流行已经夺走了近150万人的生命,病毒还在继续向全世界传播[1]. 这种疾病可以影响任何人,尽管SARS-CoV-2感染在大多数情况下会导致轻微的COVID-19,但患上严重肺炎的患者比例令人非常担忧。
众所周知,老年、肥胖、心血管疾病和糖尿病是COVID-19不良预后的危险因素[2-4.]。W.hat is not yet clear is whether chronic respiratory diseases like asthma are amongst the risk factors as well. The many studies that have addressed this question show discrepant results and point towards numerous factors that may play a role in the susceptibility and severity of COVID 19 in asthma patients [5.-10]. 这些包括哮喘本身的严重程度、哮喘表型(过敏性或非过敏性)、哮喘药物(皮质类固醇或无皮质类固醇)和共病[11-15]。B.ecause of this complex interplay between numerous factors involved, there is a need for large-scale studies that allow adjustment for confounders, making it possible to evaluate the true impact of asthma on the susceptibility and outcome of COVID-19.
这正是崔所采取的方法等等。和izquierdo.等等。在欧洲呼吸杂志的两个现实研究中[16那17]。W.hile Choi等等。included all COVID-19 cases in Korea (n=7590) by using a national claims database, Izquierdoet al。分析了71名182名哮喘患者的医疗记录数据,哮喘从西班牙区域出席医疗服务。崔等等。与一般人群相比,在Covid-19种群中发现了较高的哮喘频率(2.9与1。6–2.2%), while Izquierdo等等。found a higher frequency of COVID-19 amongst asthma patients compared to the general population (1.41与0.86%). In addition, Izquierdo等等。在生物疗法患者中表现出Covid-19的更高发病率(2.31%)。因此,这两项研究表明,在哮喘患者中对Covid-19的收缩敏感性高于一般人群,特别是在生物治疗中严重哮喘的人群。
关于Covid-19的严重程度,Izquierdo等等。报告了哮喘和非哮喘患者的等于住院率,Covid-19(两种情况26%)。同样,崔等等。found that COVID-19 severity as illustrated by ICU admission rate and duration were similar between COVID-19 patients with and without asthma. Although mortality rates were higher in patients with asthma, asthma and asthma severity did not show to be significant predictors of COVID-19 related mortality after adjustment for age, sex and co-morbidities. A higher prevalence of ICS users in patients who were hospitalised for COVID-19 was found by Izquierdo等等。,但是崔等等。未发现哮喘药物与COVID-19结局之间存在任何关联。
The studies by Choi等等。和izquierdo.等等。由于其令人印象深刻的样本量和创新方法(Izquierdo研究中的大数据分析和人工智能大数据分析和人工智能大等等。)。但是,这些大规模研究提供了我们对哮喘,哮喘和哮喘药物的严重程度影响Covid-19易感性和严重程度的明确答案吗?两项研究报告的哮喘患者中Covid-19的发病率较高或多或少与其他大(但较小)的研究一致[8.那18-20]。However, there are still some outstanding issues that may have influenced the results. First, the method by which asthma was diagnosed was very strict in the study by Choiet al。and rather vague in the study by Izquierdoet al。那possibly leading to under- or over diagnosis, respectively. This may also explain differences in proportions of patients using ICS between the two studies (23%与41%). 另一个偏倚因素可能是COVID-19的诊断方法。崔et al. 仅包括PCR证实的COVID-19病例,而Izquierdoet al。also included patients with suspected COVID-19 based on clinical parameters. In addition, infection rates may also have been affected by testing policies or shielding advices, for example, if older patients, patients with co-morbidities like asthma, or patients with more severe symptoms tested more frequently or better protected themselves. Thus, with such inaccuracies in case definition and variations in local conditions, it remains difficult to determine with certainty whether asthma patients are more susceptible to getting COVID-19 or not.
来自Covid-19的差异或死亡差的风险如何?Covid-19的严重程度和结果高度依赖年龄,因为孩子们经历严重的Covid-19比老年人更严重的Covid-19 [22]。因此,年龄是评估缔结严重Covid-19的风险的重要混乱。Izquierdo.et al。showed that asthma patients without COVID-19 were younger and more likely to have eczema and rhinitis, while those with COVID-19 were older and more likely to have co-morbidities like hypertension and diabetes. These results could very well be confounded by age. Choiet al。solved this issue by adjusting for age and co-morbidities in a multivariate analysis, which would have been of additive value in the study by Izquierdoet al。
W.hat do the two studies teach us about safety of asthma medication, in particular inhaled corticosteroids with respect to COVID-19 susceptibility and outcome? There is much debate about the risk-increasing or protective effects of asthma medication in the course of COVID-19 disease [23]. 在这种风险评估中,哮喘的严重程度和表型是重要的混杂因素。崔et al。found higher health-care related costs in patients using oral short-acting beta agonists (SABA). However, less than 4% of patients used oral SABA in the 2 months before COVID-19 diagnosis, suggesting that not oral SABA itself, but other factors, such as the type of patients that is prescribed oral SABA, played a role in these increased costs. Not surprisingly, regression analysis showed that asthma medications were not independently associated with poor outcome of COVID-19. Choi等等。还发现接受第5步治疗的患者住院时间更长(定义为前一年口服皮质类固醇≥90天),但由于只有4名患者接受第5步治疗,因此无法得出确切结论。伊斯基耶多et al。得出结论,ICS使用是“安全”,因为其研究中的ICS用户比非ICS-Users为Covid-19的频率较少。然而,该发现与英国最近的观察性研究表现出哮喘患者在哮喘患者中较高ICS剂量和Covid-19相关死亡风险之间的关联[13]。The studies by Choiet al。和izquierdo.等等。没有考虑到的剂量ICS,这可能吗partly explain the discrepancy between the three studies regarding the influence of ICS use on COVID-19 outcome.
How about the use of asthma biologics and the risk of COVID-19? Currently available asthma biologics block pathways of type 2 inflammation This type of inflammation, in particular allergic inflammation, has been suggested to have a protective effect through down-regulating the angiotensin converting enzyme (ACE)2 receptor used by the virus to enter host cells, or hypothetically, by counterbalancing the exaggerated anti-viral immune response observed in severe COVID-19 patients [24那25]。Izquierdo.et al. 对大量接受生物治疗的患者(n=865)进行分析,发现COVID-19在这些患者中的发病率相对较高,为2.3%,而在一般哮喘人群中的发病率为1.4%。使用哮喘生物制剂的20名感染者中只有2名(10%)住院。虽然这些数字很小,但它们与其他报告一致,这些报告表明使用生物制剂的哮喘患者预后不良的风险没有增加[21那26]。
总之,这些大规模的研究证实了先前关于哮喘患者发展(严重)COVID-19风险的发现。哮喘患者似乎更容易感染COVID-19,但严重的疾病进展似乎与药物使用(包括哮喘生物制剂)无关,而是与年龄和共病有关。
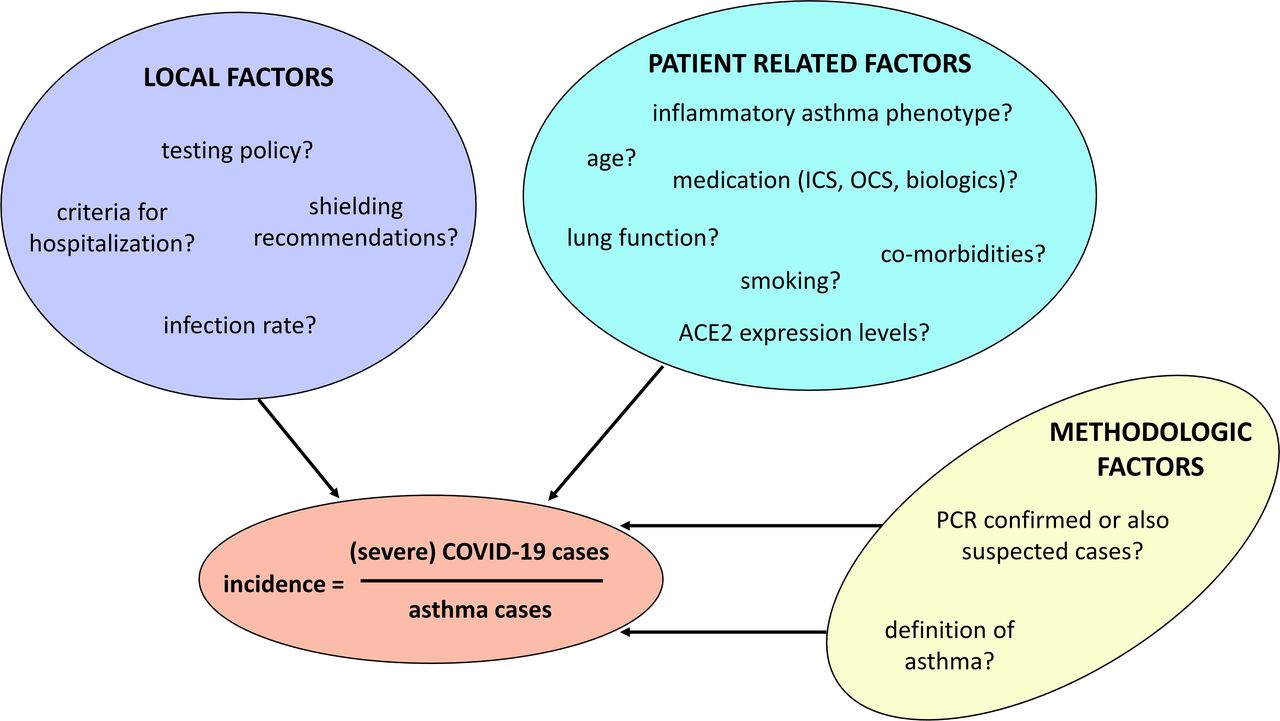
However, no definitive conclusions can be drawn yet as many factors can influence the reported incidences of (severe) COVID-19 (图1). 到目前为止,这些潜在的偏倚因素在已发表的研究中还没有得到考虑,因此许多问题仍然没有答案。类似的大规模的,最好是跨国的真实生活研究,详细说明确诊为COVID-19的患者的哮喘表型和药物使用情况,将是进一步建立在这一新证据基础上的理想下一步。
可能影响哮喘患者(严重)COVID-19发病率的因素。图例图1:报告的哮喘患者中的(严重)Covid-19病症的发病率并不是由患者相关因素确定的。当地因素和所应用的方法也可以发挥重要作用。缩写:ACE2,血管紧张素转换酶2;Covid-19,冠状病毒疾病2019;IC,吸入皮质类固醇;OCS,口服皮质类固醇。
Conflict of Interest Statement: KE has nothing to declare. EHB Dr. Bel reports grants and personal fees from AstraZeneca, grants and personal fees from GSK, grants and personal fees from Novartis, personal fees from Sanofi/Regeneron, grants and personal fees from Teva, personal fees from Sterna, personal fees from Chiesi, outside the submitted work.
Footnotes
Conflict of interest: Dr. Eger has nothing to disclose.
利益冲突:Bel博士报告Astazeneca的赠款和个人费用,GSK,赠款和个人费用从Novartis,Sanofi / Regeneron的个人费用,Teva的赠款和个人费用,斯得人的个人费用,个人费用来自Chiesi,在提交的工作之外;
- Received德cember 8, 2020.
- 公认德cember 16, 2020.
- 版权所有©ERS 2020
本文是开放获取的,并根据知识共享188滚球软件署名非商业许可4.0的条款分发。











{kind=link}
{kind=link}