





Abstract
Hands can be vehicles for of transmission of pneumococcus leading to nasopharyngeal colonisation, even after dryinghttp://ow.ly/svlu30liKqP
到编辑:
S.treptococcus pneumoniae(pneumococcus) is a major cause of acute otitis media, sinusitis, pneumonia and meningitis worldwide [1]。超过120万婴儿死亡归因于S.。pneumoniae每年 [2]。
Colonisation of the human nasopharynx with pneumococcus is common, with prevalence between 40% and 90% in children <5 years old and approximately 10% in adults in cross-sectional surveys [3.]。Colonisation is important as it is a pre-requisite to infection, the primary reservoir for transmission, but can also boost immunity [1那4.]。
It is postulated that transmission ofS.。pneumoniaeoccurs primarily by indirect contact通过inhalation of airborne droplets. Supporting this are observations that transmission is associated with higher density living (day care centres, prisons and nursing homes), and is enhanced by concurrent viral respiratory tract infections [5.]。For upper respiratory tract infections in general, direct contact is implicated in disease transmission, which can be interrupted by hand washing [6.]。However, the relative contribution of direct and indirect transmission modes to pneumococcal colonisation and disease are unknown. We aimed to assess the potential for pneumococcal hand-to-nose transmission to cause nasopharyngeal colonisation.
W.e enrolled 63 healthy adult participants, between April and May 2017, to our controlled Experimental Human Pneumococcal Challenge model (EHPC), modified slightly from previous published protocols to assess “hand-to-nose” [7.]。
B.riefly, participants were administered pneumococcus (3.2×106.mid-log phase colony-forming units (CFU) ofS.。pneumoniaeserotype 6B prepared as previously described) onto their fingertip or dorsum of their hand [7.]。通过血琼脂的细菌储备连续稀释(Sokoid,BasingStoke,UK)通过细菌密度证实了细菌密度。要求参与者嗅到细菌残留物或与鼻粘膜表面直接接触(挑选/戳鼻子),并在暴露后立即(“湿”)或明显干燥(约1-2分钟接触后)。在肺炎球菌暴露之前进行基线筛选;在暴露之前,与肺炎骨膜自然殖民的参与者被排除在外。咽喉前喉咙拭子也用于呼吸道病毒(腺病毒,流感A和B,冠状病毒,呼吸道和平病毒/人颅骨病毒,鼻病毒和Parainfluenza 1-4),如前所述的[8.]。
All participants were followed up for 9 days after exposure. Nasopharyngeal colonisation was assessed in nasal washes collected at days 2, 6 and 9. Pneumococcal density in nasal washes was determined by culture in real time; serotype was determined as 6B using a latex agglutination kit (Statens Serum Institute, Copenhagen, Denmark). Following completion of the study all samples were tested by quantitative PCR (qPCR) with primers forLyta.那and forS.。pneumoniaeserotype 6A/B. Rates of pneumococcal acquisition between groups were compared using Fisher's exact test.
All participants gave written, informed consent. Ethical permission was granted by the local National Health Service Research Ethics Committee (17/NW/0054).
B.etween March and June 2017, 76 participants were recruited for the hand to nose study (ISRCTN: 12909224), with 63 participants completing all the study visits. The mean age of volunteers was 22.6 years of age (range 18–45, median 21 years) and the male:female ratio was 23:40.
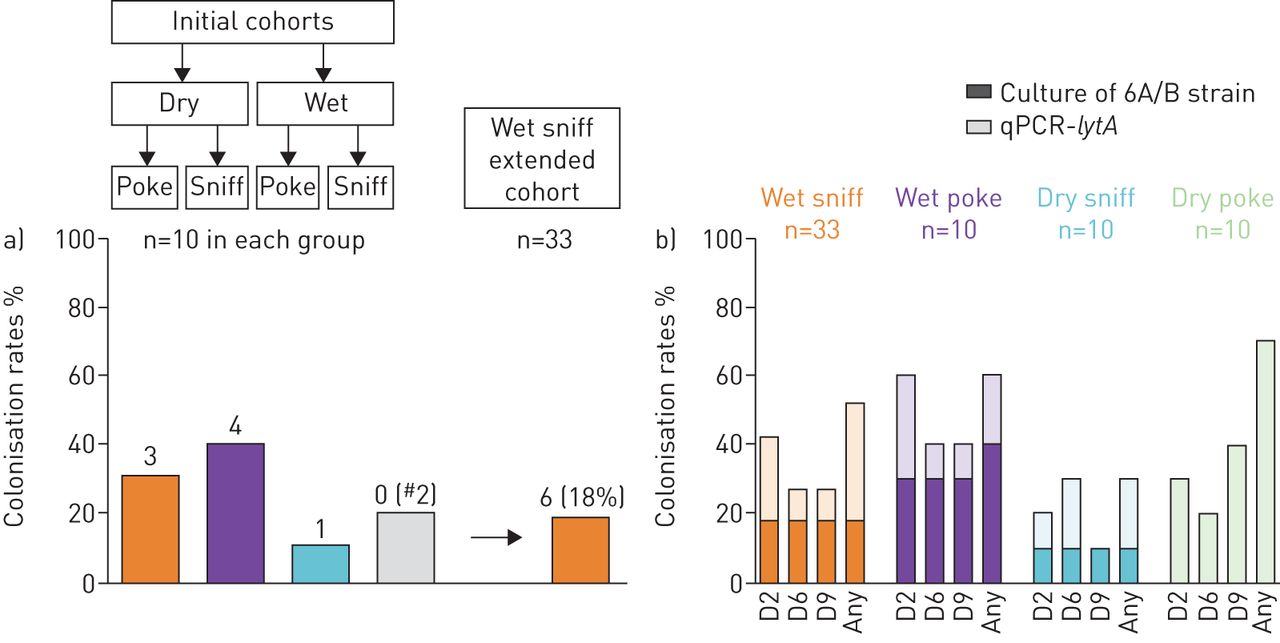
4.0 participants were initally randomly allocated to four different transmission groups: 1) sniffing wet bacterial suspension (“wet sniff”); 2) sniffing bacterial suspension after air-drying (“dry sniff”); 3) pick/poke nose with finger exposed to wet bacterial suspension (“wet poke”); and 4) pick/poke nose with finger exposed to bacterial suspension after air-drying (“dry poke”).
在这一初始群组中,40名参与者,发现八(20%)在培养的后续访问时用肺炎球菌(6B)进行实验殖民,在“湿戳”(4/10,40%)中,和“湿嗅”(3/10,30%)组。在“嗅探”或“戳”之前,允许细菌在皮肤上干燥,分别为1/10和0/10参与者进入殖民(figure 1)。四种不同的群体太小而无法比较,分析潮湿versusdry groups highlighted that colonisation rates in the “wet” group were significantly higher than the “dry” group (p=0.04, Fisher exact test).
{kind=link}
{kind=link}
a) Colonisation rates following classical culture of nasal wash samples at any time point after exposure in each transmission group.#:no experimental carriers of strain 6B found in dry poke group but two participants became natural carriers of pneumococci after exposure to 6B. b) Comparison of culture (6A/B strain only) andLyta.quantitative PCR (qPCR) results for different transmission methods.
“湿嗅”,“湿戳”和“干嗅”组的中位曝光后殖民化密度(CFU / ml鼻腔洗涤)为5.6×101(range 4.3×10-1to 3.7×106.), 4.7 (range 4.5×10-1to 1.3×102) and 2.4 (range 1.2 to 9.6) respectively. Following the culture results the “wet sniff” group was expanded to improve precision estimates of rates, this group was expanded due to the combination of good colonisation rates and high density of colonisation episodes in participants. A total of 6/33 volunteers became colonised (18%). No viruses were detected in any throat swabs taken before pneumococcal exposure.
molecular detection (Lyta.qPCR) identified higher colonisation rates compared with culture (whole cohort evaluated: 33/63 (52%)versus13./6.3.(23%), respectively; p<0.0001, Fisher's exact test) (figure 1)。T.his was most apparent in “dry poke” group; colonisation in 0/10 by culture and 7/10 using qPCR. Samples which were only positive with qPCR tended to have lower densities of carriage compared to samples positive with both methods. Higher densities were noted in the wet sniff group and in samples that were carriage positive with both methods.
T.he study shows for the first time, using a controlled human infection model, that the hands can be a vehicle for transmission of pneumococcus and lead to acquisition of nasopharyngeal colonisation.
T.his novel use of a human challenge model allowed for the study of pneumococcal transmission and colonisation in a controlled environment. Previous pneumococcal challenge studies have directly inoculated bacteria into the noses of participants. This direct exposure method with 6B serotype has resulted in a colonisation rate of approximately 45% using culture detection method [3.那4.]。人体挑战模型的定植率可能依赖于各种宿主和细菌因素,包括宿主免疫。该研究的较低的殖民率可能是由于嗅探传动方法导致病原体从鼻咽中移动或由于在手中的干燥过程中的肺炎球菌死亡而导致。
Pneumococcal survival on the skin has been reported, with persistence of viable bacteria for 3 h following exposure [9.]。W.e have further shown that pneumococcus can survive drying on the skin, and go on to cause colonisation. An association between frequent sharing of drinking glasses or bottles and pneumococcal colonisation has also been reported [10]。作者表明,这些发现表明,通过唾液的肺炎球菌传播是年轻人的高度合理的路线,然而,不考虑或研究手中的手可以是这种传输的载体的可能性。在这项研究的结果之后,可以似乎可以涉及手动污染和手鼻传递,可以涉及“经常共享组”中看到的殖民化率较高。
Our results support other studies in suggesting that determining pneumococcal colonisation by both culture and qPCR are complementary [11那12]。Higher rates of detection using molecular methods likely represent superior sensitivity at low-density colonisation. Of those only detectable by qPCR, all had densities below 103.copies per mL. The main limitation is the inability to distinguish viable from non-viable bacteria, potentially causing false-positive results [3.]。
L.imitations of the study include the use of a young healthy adult population. Children are the primary reservoirs for community pneumococcal transmission, although an adult population was used in this study, the results suggest the potential for hand-to-nose transmission in paediatric populations [2]。参与者的短暂的后续行动期限限制了我们的能力,评估了殖民化和不同传输方法的持续时间影响殖民化的寿命。用于暴露的细菌库存源自培养基,是中木阶段;这些实验条件可能影响肺炎球菌活力和定植势。最后,我们只研究了自我接种的肺炎球菌的潜在传播;检查肺炎球菌蔓延的相对风险通过aerosolised bacteria, direct contact or indirect contact would be beneficial, similar to previous studies investigating transmission of respiratory viruses [13.]。
W.e were unable to investigate the relationship between colonisation acquisition and concurrent viral infection due to the absence of viral infection in our participants, probably due to seasonality. In a previous study, asymptomatic co-infection increased the odds of experimental pneumococcal colonisation (75% virus positive participants became colonisedversus4.6.% virus negative; p=0.02), and other experiments have shown that viruses (such as rhinovirus) facilitate acquisition and transmission between individuals [8.那14.]。
T.his study is the first to show that direct pneumococcal transmission can occur leading to colonisation acquisition. Good hand hygiene practices, already known to reduce enteric bacterial and viral disease, may also prevent the spread of bacteria thought to be primarily spread through aerosolisation. Follow-on experimental trials would be needed to examine whether true person-to-person transmission could occur with pneumococcus moving from the hands into the nose efficiently enough to cause colonisation. This supports advice about cross-infection risk in patients with bronchiectasis from Chalmers等等。[15.]。建议我们high-risk patients to practise rigorous hand hygiene, to avoid shaking of hands and ensure basic infection control measures, such as avoidance of sharing food, drink and mobile phones, may reduce the transmission of respiratory bacterial pathogens such as pneumococcus. For healthy adults and children, it is unclear if reducing exposure to pneumococcus would be beneficial for overall health; pneumococcal exposure and colonisation have been shown to elicit immune responses which may be beneficial in later life [4.那16.]。
更好的理解生存的持续时间f pneumococci in nasal secretions on the hands and the frequency of hand contamination would help understanding of the transmission process further. Studies to improve knowledge about the process of pneumococcal shedding from the nose in humans during colonisation, and factors which promote shedding, are also warranted. This modification of the EHPC model has several potential uses, including testing of current or new hand cleaning interventions to ensure reduction in transmission of this important bacterial pathogen.
Acknowledgements
T.he authors thank the respiratory research team; trial steering committee members; Stephen Gordon, Malawi–Liverpool–Wellcome Trust Clinical Research Programme; clinicians who provided safety on-call cover; John Blakey, Steve Aston and Ben Morton, and the Liverpool School of Tropical Medicine (LSTM) respiratory group.
Footnotes
该研究在具有标识符12909224的ISRCTN中注册。
兴趣冲突:V. Connor报告在研究中的联合利华的赠款;该研究由联合利华部分资助,他参加了研究设计。研究,分析和介绍的结果,以及发布的决定仅由作者确定,没有任何资金来源的影响。
Conflict of interest: E. German reports grants from Unilever and Medical Research Council, during the conduct of the study.
Conflict of interest: S. Pojar reports grants from Unilever and MRC, during the conduct of the study.
利益冲突:E. MITSI没有什么可披露的。
Conflict of interest: C. Hales reports grants from Unilever, during the conduct of the study; the study was part-funded by Unilever, who participated in the study design. The conduct of the study, analysis and presentation of results, and decision to publish were solely determined by the authors, without influence from any funding source.
Conflict of interest: E. Nikolaou has nothing to disclose.
Conflict of interest: A. Hyder-Wright reports grants from Unilever, during the conduct of the study; the study was part-funded by Unilever, who participated in the study design. The conduct of the study, analysis and presentation of results, and decision to publish were solely determined by the authors, without influence from any funding source.
Conflict of interest: H. Adler reports grants paid to institution from Unilever, during the conduct of the study.
Conflict of interest: S. Zaidi has nothing to disclose.
兴趣冲突:H. Hill无需披露。
Conflict of interest: S.P. Jochems has nothing to disclose.
Conflict of interest: H. Burhan has nothing to disclose.
兴趣冲突:在研究期间,N.法国报告从联合利华PLC拨罪(利物浦大学支付给了Liverpool大学)。
利益冲突:T. Tobery是联合利华的全职雇员,为这项工作提供了资金;然而,T. Tobery从联合利华的赔偿不受此处描述的工作或出版物的影响。
Conflict of interest: J. Rylance has nothing to disclose.
Conflict of interest: D.M. Ferreira has nothing to disclose.
S.upport statement: This work received financial support from Unilever and The Medical Research Council (MRC). Funders did not have any input into the study design. Funding information for this article has been deposited with theCrossref Funder Registry。
- R.eceivedmarch 27, 2018.
- 公认August 1, 2018.
- 复制right ©ERS 2018
R.eferences










