





抽象的
通过治疗难以治疗XDR-TB的患者跨越边界;高度个性化但整体的方法http://ow.ly/jyjk30ielsd
致编辑:
Extensively drug-resistant (XDR) tuberculosis (TB) is defined by resistance to isoniazid, rifampicin, any fluoroquinolone and at least one of the three second line injectable drugs, such as amikacin. Drug toxicity and duration impair adherence to treatment and outcome is rather poor [1]。我们报告了一名特别具有挑战性的XDR-TB患者,对治疗持续不遵守和异常复杂的药物敏感性模式。
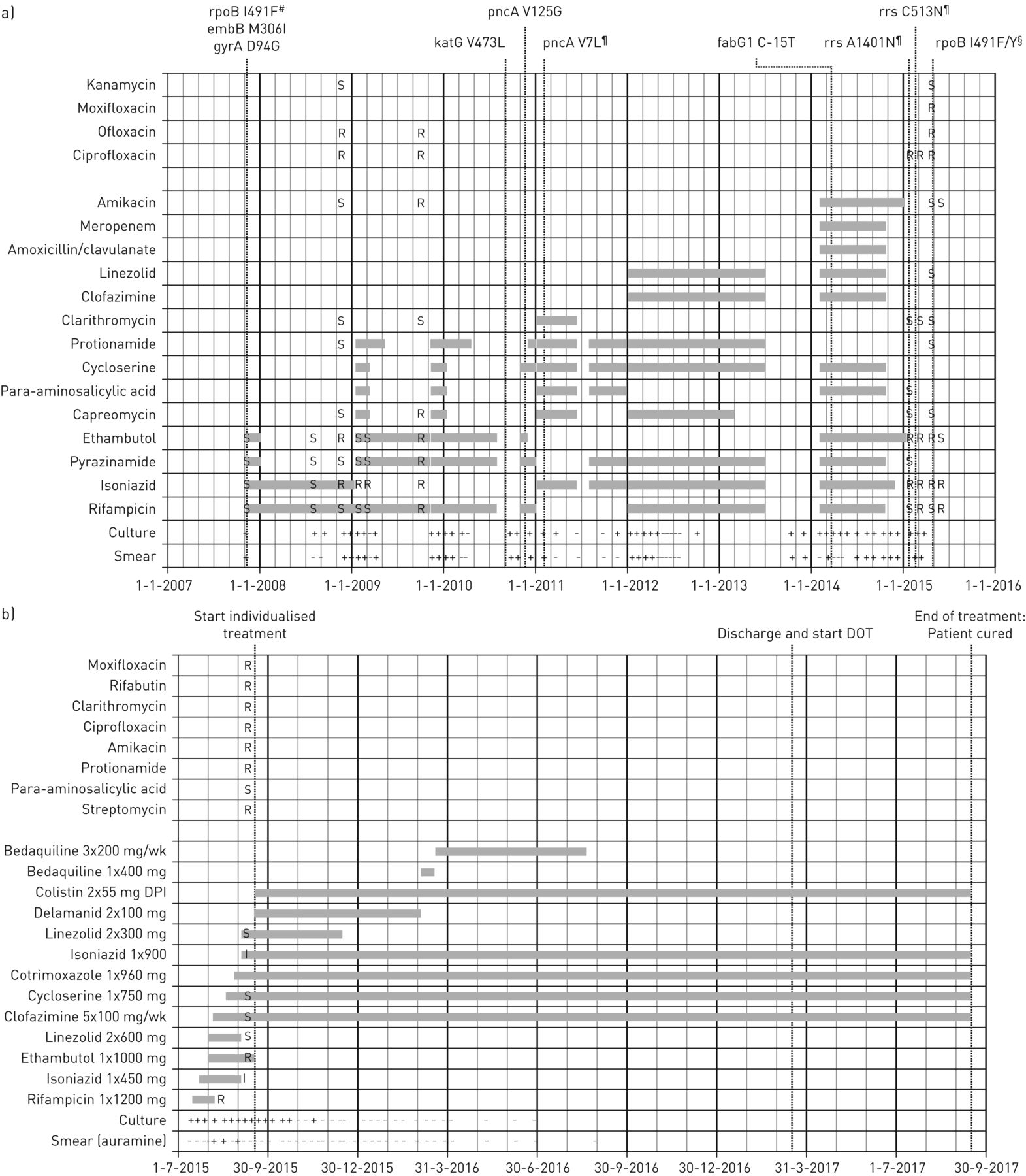
2015年7月7日,一名拥有XDR-TB的28岁英国公民从英国转移到荷兰Haren的结核病中心“ Beatrixoord”中心。他没有其他相关的合并症和艾滋病毒和慢性肝炎的阴性测试。他的父亲最初在1999年被诊断出患有药物敏感的结核病,并于2005年屈服于多药耐药(MDR)TB。尽管2000年在Isoniazid进行了预防治疗,但该患者于2007年11月开始诊断出患者患有药物敏感的结核病。一线结核病治疗。在7年以上的过程中,许多医院入院,而他的结核分枝杆菌分离株变得越来越耐药,他的治疗方案曾经扩展(图1A)。尽管经常进行分子和表型耐药性测试,即使进行了整个基因组测序(WGS),但几种药物的结果还是模棱两可的。到2009年底,他的结核病被归类为广泛的耐药性。2011年中期,在2012年再次获得了两种连续的阴性培养物,但两次都进行了培养(随后培养)(图1A)。Our patient was addicted to cannabis and had many social problems resulting in poor adherence to therapy. Other possible causes of a failing regimen, like poor drug absorption, were considered, but at that time it was believed that the extremely poor adherence was the major problem. In mid-2015, his medical team felt that only a highly individualised treatment regimen focusing not only on pharmacotherapy, but also on a change in social environment and social habits might curb impending fatal outcome. This was difficult to realise in the UK, because the Public Health Act lacks a compulsory treatment order and sanatoria are not available. The TB centre in Groningen, the Netherlands provides an environment conducive to long-term treatment of socially complex and medically challenging TB cases. In addition, the Dutch Public Health Act enables long-term mandatory isolation of patients unwilling to follow infection control procedures. Our TB centre and the Dutch national health authorities were approached by the National Health Service (NHS) to discuss the patient's transfer. The health authorities of both countries supported the transfer and the NHS and our TB centre agreed on the conditions, including financial arrangements, and the patient gave his consent.
时间轴包括药物治疗,痰液测试结果以及对a)英国和b)荷兰治疗的药物敏感性测试的结果。#:编码低水平利福平抗性的有争议的突变;¶:混合野生型/突变体;§:在含有高浓度利福平或amikacin的琼脂菌落分离后发现高水平利福平抗性的RPOB基因中的混合第二突变。S:易感性;R:抗性;I:中级抗性;+:积极;- :负;DPI:干粉吸入;点:直接观察到治疗。
此后的头几个月,美国国家公共卫生与环境研究所(RIVM,Bilthoven,荷兰)对当前和以前进行了药物敏感性测试(DST)结核分枝杆菌痰分离物。基于第一个测试结果,我们开始使用高剂量利福平,异念珠菌,ethambutol,cycloserine和linezolid治疗[2]。进行治疗药物监测(TDM)以优化治疗[3]。进一步的分析揭示了几个少数人群的存在结核分枝杆菌对利福平和amikacin具有模棱两可的敏感性。然而,在从7H10琼脂分离出最高浓度的这两种药物(2和5 mg·L-1respectively) [4]。在这些分离的菌落中,分子靶标(RPOB(ATC 491 TTC→TAC)和RRS确定了所有药物的基因(A1401→G))以及所有药物的全部药物敏感性谱。最初未被WGS未发现的高度利福平和抗氨基酸抗性少数族裔具有相似的抗药性特征。对抗性谱的分子分析显示,在未经药物选择的后来培养菌株中,具有高度抵抗力的少数群体,这表明它们的数量随时间增加。由于发现该药物的高累积最小抑制浓度,因此停用了利福平。基于较早的研究[5],每天将960 mg共曲唑唑一次添加到该方案中。此外,等剂量增加到900 mg。根据DST结果,只有很少的有效药物可用,我们以连续的顺序添加了Delamanid和Bedaquiline。对于早期的培养转换,我们考虑添加另一种药物。甲前唑酮的可用性差,因此我们选择了吸入的结肠素。体外研究表明,结肠素的异oni偶抑制作用[6,,,,7], and it was shown that the required colistin concentrations in sputum to achieve such effects could be reached by dry powder inhalation [6,,,,8]。We used the Twincer® dry powder inhaler (PureIMS, Roden, the Netherlands) to minimise adverse reactions such as cough [8,,,,9]。我们指示正确吸入功效。仅观察到linezolid的不良药物反应,在患者开始发展周围神经病后,该反应被停用。图1B提供了给定的药物治疗方案的概述。由于双边参与,肺部储备不足和广泛的疤痕,因此在技术上认为手术切除是一种补充治疗。
除了改变药房治疗外,荷兰结核病中心还提供了身体和社会环境的变化,帮助我们的患者遵守治疗。他不仅脱离了他复杂的社交生活,而且还可以为他提供量身定制的几项社交和身体日常活动。
With the support of the nursing staff, he managed to adhere to therapy and within 2 months of the start of his tailor-made drug treatment, his sputum smear and culture converted negative (图1B)。经过18个月的住院治疗,他继续在格罗宁根(Groningen)的门诊治疗,荷兰在我们的结核病中心直接观察到5天的治疗。在24个月之前考虑治疗完成。上肺叶的双侧放射学异常持续存在,没有任何并发症。
取得成功,几个边界交叉。First, moving the patient far away from his social environment that precluded treatment adherence was crucial. Second, his transfer to the TB centre enabled him to follow an individualised social programme in a hospitable physical environment that helped him to comply with treatment. Third, the problem of highly complicated molecular and phenotypic DST results was solved by isolating the most resistant bacteria on DST agar plates. All relevant resistance profiles of the causative bacteria were disclosed and therapy could be tailored and adjusted accordingly. Despite using cutting edge technology including WGS, initial DST predictions failed because of minority bacterial populations hidden by abundantly present susceptible bacteria. We speculate that highly resistant minority bacterial populations may be critical in patients with a long treatment history. Fourth, TDM helped to optimise treatment with the limited pharmaco-therapeutic options available. We targeted drug concentrations within the therapeutic window, thereby reducing toxicity and increasing the chance of a favourable outcome [10]。
最后,我们能够通过几种实验药物扩展我们的方案。除了添加Delamanid,Bedaquiline和Co-Trimoxazole,这是一种具有合理安全性和有效性的药物[5],我们是第一个在该患者中施用大肠杆菌蛋白干粉末吸入高剂量异念珠菌的人。已经假设,通常,亲水性抗生素可以受益于大肠菌素的这种增强作用[6],因此,环丝氨酸(logP = -0.9)也可能已经增强。
Close collaboration between all stakeholders in the treatment of MDR- and XDR-TB in the Netherlands has resulted in a treatment success rate as high as that of drug-susceptible TB [11,,,,12]。大多数来到荷兰市政卫生服务部结核病部门的患者都是外国出生的。结核病单元已收到具有不同语言和文化背景的患者。国家计划已经在跨境中共同努力,但他们也可能考虑共享高度专业化的资源良好的设施来治疗高度复杂的结核病案例。
脚注
利益冲突:F。Grasmeijer在提交的工作之外报告了Pureims BV的兼职工作。
利益冲突:H.W.Frijlink拥有呼吸驱动的干粉吸入器的专利(数字WO 2015/187025 A1)。
利益冲突:P。Hagedoorn拥有申请专利,是Twincer的共同发明人。
利益冲突:T.S.Van der Werf是RUTI治疗疫苗试验的首席研究员,部分由西班牙Badelona Archivel赞助;并参加了由TBVI在2016年6月组织和赞助的会议,并参加了TBVI组织并于2017年11月由Transgene -Institut Merieux组织的会议。
- 已收到2017年12月1日。
- 公认2018年1月20日。
- 版权所有©ERS 2018
this ERJ Open article is open access and distributed under the terms of the Creative Commons Attribution Non-commercial Licence 4.0











{kind=link}
{kind=link}