





Abstract
Mesothelin has been proposed as a useful tool in the diagnosis of malignant pleural mesothelioma (MPM). We aimed to examine its diagnostic utility and the impact of renal impairment on results.
We prospectively recruited 230 patients with new undiagnosed pleural effusions, testing serum (n=216) and pleural fluid (n=206) mesothelin (by ELISA) during the initial consultation.
28 (12%) out of 230 patients had MPM. Serum mesothelin gave sensitivity 59.3%, specificity 64.7%, negative predictive value (NPV) 91.2%, positive predictive value (PPV) 20.5%, and pleural fluid sensitivity 72.0%, specificity 87.5%, NPV 95.5%, PPV 46.2% for distinguishing effusions due to MPM. In a matched comparison, diagnostic characteristics of pleural fluid mesothelin were superior to serum (p=0.0001). Serum mesothelin levels in patients without MPM were higher in patients with renal impairment (p=0.007) while pleural fluid levels were unaffected. 19 (54%) out of 35 patients with a benign pleural effusion and an estimated glomerular filtration rate ≤59 mL·min−1had a false-positive serum mesothelin result.
The diagnostic accuracy of pleural fluid mesothelin is superior to that of serum and is unaffected by renal function. In patients with a low pre-test probability of mesothelioma, a negative mesothelin test could be reassuring, because of its high NPV. Routine use of mesothelin testing in undiagnosed pleural effusions at presentation appears to be unhelpful.
Malignant pleural mesothelioma (MPM) is an increasingly common malignancy worldwide with a predicted peak in incidence between 2015 and 2025 in many countries [1]。Most patients present with a pleural effusion and associated breathlessness, a clinical picture with a wide range of possible malignant and benign aetiologies [2]。The diagnosis of MPM can be elusive, particularly in frail patients who are unfit for the most invasive of available diagnostic procedures such as video-assisted thoracoscopy and biopsy [3]。Pleural fluid cytology is of low sensitivity and discrimination between mesothelial cellular atypia due to inflammation and MPM can be challenging [4]。Computed tomography (CT) scan appearances, while of reasonable specificity for identifying malignant thickening of the pleura, distinguish poorly between MPM and adenocarcinoma [5]。
A history of asbestos exposure is common amongst patients presenting with a new pleural effusion, many of whom are ultimately diagnosed with benign disease but must be investigated extensively to exclude a malignant diagnosis [3]。在particular, the diagnosis of benign asbestos-related pleural effusion (BAPE) can currently only be made with confidence following benign pleural biopsy and prolonged radiographic follow-up [6]。
Serum or pleural fluid biomarkers that could rule out MPM in high-risk groups, accurately raise diagnostic suspicion in lower risk patients and/or clarify non-diagnostic test results would be valuable.
There have been several studies examining the use of serum mesothelin, a 40-kDa glycoprotein product of mesothelial cells, as a diagnostic and/or screening tool for mesothelioma, and a recent meta-analysis concluded summary estimates of 64% sensitivity and 89% specificity [7] for the test, which can be performed as a commercially available ELISA. Most studies have employed tissue bank samples, selecting defined diagnostic sub-groups rather than true consecutive series of patients presenting in clinical practice.
The two largest studies to date, examining the use of pleural fluid for mesothelin testing, gave sensitivities of 67% and 71% and specificities of 98% and 89% for the diagnosis of mesothelioma [8,9]。Davieset al.[9] demonstrated promising diagnostic characteristics for pleural fluid mesothelin in the clarification of non-diagnostic pleural fluid cytology.
Renal impairment has recently been shown to be an independent predictor of elevated serum mesothelin in patients without pleural disease and false-positive rates of >50% have been shown in control populations with stage 3 chronic kidney disease (CKD) or greater [10,11]。A further study by Hollevoetet al.[12] demonstrated an independent association between age, glomerular filtration rate and body mass index and serum mesothelin. The effect of clinical variables such as renal function on mesothelin levels in pleural fluid has not been fully explored.
The aim of the current study was to apply serum and pleural fluid mesothelin testing to a “real-world” prospective consecutive series of patients presenting with an undiagnosed pleural effusion and examine diagnostic utility throughout the standard investigation pathway, compare accuracy between serum and pleural fluid and establish the impact of renal impairment on results.
MATERIALS AND METHODS
The study was approved by North Bristol NHS Trust Research Ethics Committee, Bristol, UK (08/H0102/11).
Consecutive patients presenting to the pleural disease service of a large UK teaching hospital between July 2008 and July 2010 with an undiagnosed pleural effusion requiring investigation were approached for consent. All recruited patients gave informed written consent.
All patients underwent a comprehensive clinical assessment adhering to British Thoracic Society Guidelines [6]。
Cytology/histology techniques and CT scan reporting protocol are described in the online supplementary material.
Clinical data collection
Clinical data were collected prospectively throughout the patients’ involvement in the study. Case notes were reviewed a further 12 months after trial entry to establish the final diagnosis.
Mesothelin quantification
Paired serum and pleural fluid samples were collected in serum gel separator tubes and centrifuged at 1,000×g for 20 min. The supernatant was stored at -70°C for later assay. Mesothelin concentrations were measured with a commercially available ELISA (Mesomark®; Fujirebio Diagnostics Inc., Malvern, PA, USA). Clinical team members were blind to the mesothelin results.
Method of estimated glomerular filtration rate (eGFR) calculation is given in the online supplementary material.
Final diagnosis and follow-up
Patients were followed-up to a histological or microbiological diagnosis, to complete resolution of the pleural effusion, to death or for a minimum of 12 months. The final diagnosis of each effusion was established independently by two consultant chest physicians using predefined diagnostic criteria by comprehensive review of investigation results and case notes, blind to the mesothelin result. Patients who did not fulfil any diagnostic category following exhaustive investigation and 12 months follow-up were considered “undiagnosed”. Full diagnostic criteria are described in the online supplementary material.
Statistical analysis
Analyses were performed using STATA (StataCorp, College Station, TX, USA) version 12.0 and Prism (GraphPad Software, La Jolla, CA, USA) version 5.0. Differences in the distribution of serum mesothelin and pleural fluid mesothelin levels were compared between patients with and without MPM. Due to the non-normality of the data (based on the D'Agostino–Pearson omnibus normality test), the Mann–Whitney U-test was used to compare medians.
The diagnostic accuracy of serum and pleural fluid was then compared first using a fixed specificity of 95% (obtained from a receiver operating characteristic (ROC) analysis), including patients for whom both sample types was available, and secondly, including all available results, using pre-defined cut-off levels that have been previously recommended for use in practice. Serum testing used the test manufacturer's cut-off level of 1.5 nM and pleural fluid testing used the best cut-off established in previous studies of 20 nM [8,9,13]。95%置信区间的措施of diagnostic accuracy. Non-parametric ROC curves were obtained, and the area under the curve (AUC) was compared between serum and pleural fluid for the paired data. Patients who were undiagnosed or had “radiographic only” diagnoses of malignancy were excluded from all analysis of diagnostic accuracy.
A sub-group analysis was performed to determine whether significant CKD affected test results. Patients were classified into groups based on eGFR results (≤59 mL·min−1(stage 3 CKD or greater)versus>59 mL·min−1), and the two groups were compared in terms of sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV).
RESULTS
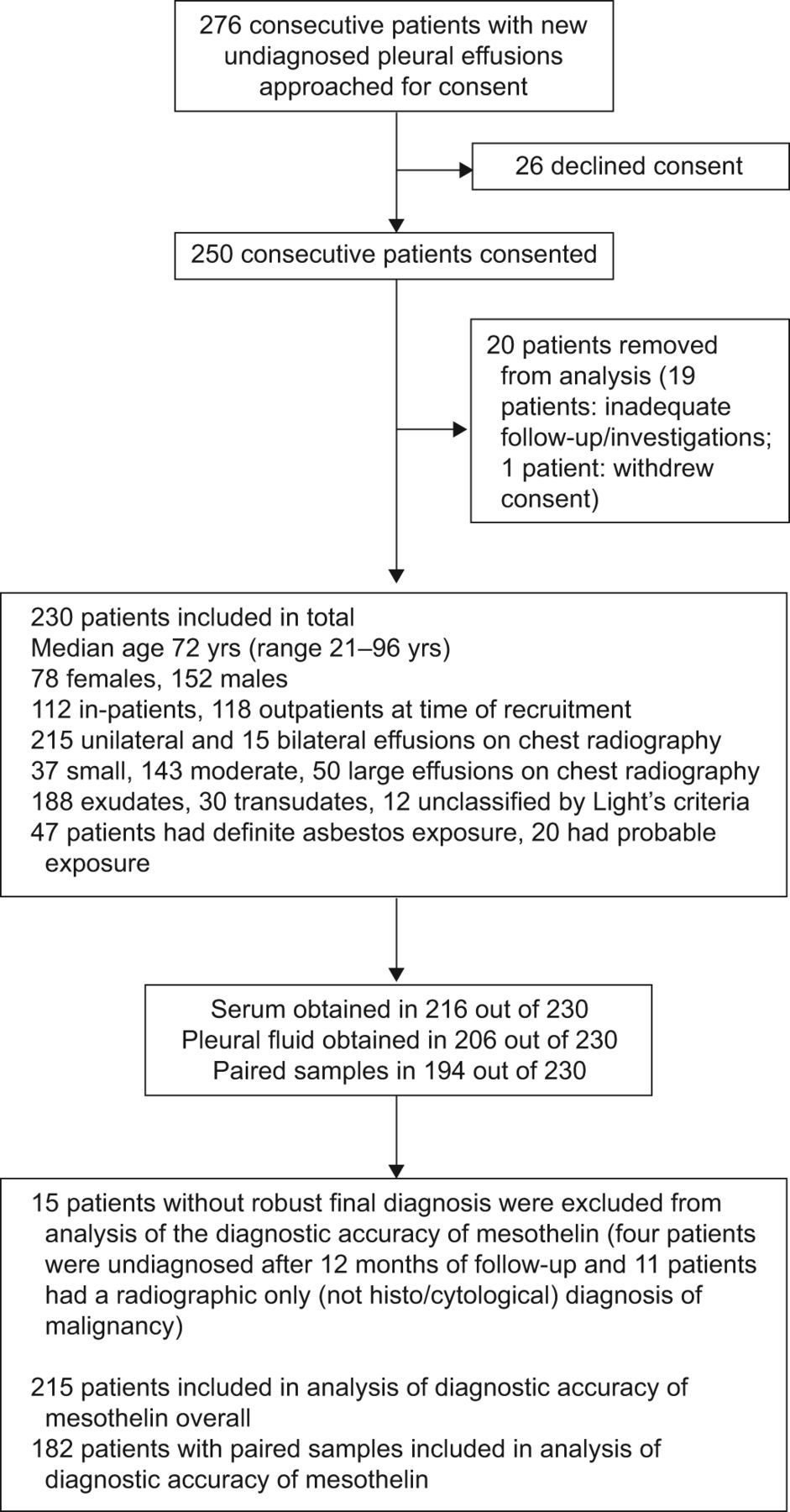
Patient recruitment, inclusions, exclusions and demographics are detailed infigure 1.
{kind=link}
{kind=link}
Patient recruitment, inclusions, exclusions and demographics.
Agreement between reviewing consultants with regards to the final diagnosis for cause of effusion was good with an un-weighted κ concordance score of 0.96 (95% CI 0.93–0.99).
Table 1summarises patient diagnoses and mesothelin levels.
Serum and pleural fluid mesothelin levels in diagnostic patient sub-groups
The median (interquartile range) serum mesothelin level amongst patients with MPM (n=27) was 2.10 (0.80–6.91) nM, significantly greater than in those with confirmed non-MPM diagnosis (n=176) (1.17 (0.90–1.91) nM; p=0.04). Median pleural fluid mesothelin level in patients with MPM (n=25) was 41.2 (14.7–70.0) nM, also significantly greater than non-MPM patients (n=168) (5.90 (2.85–11.0) nM; p<0.0001).
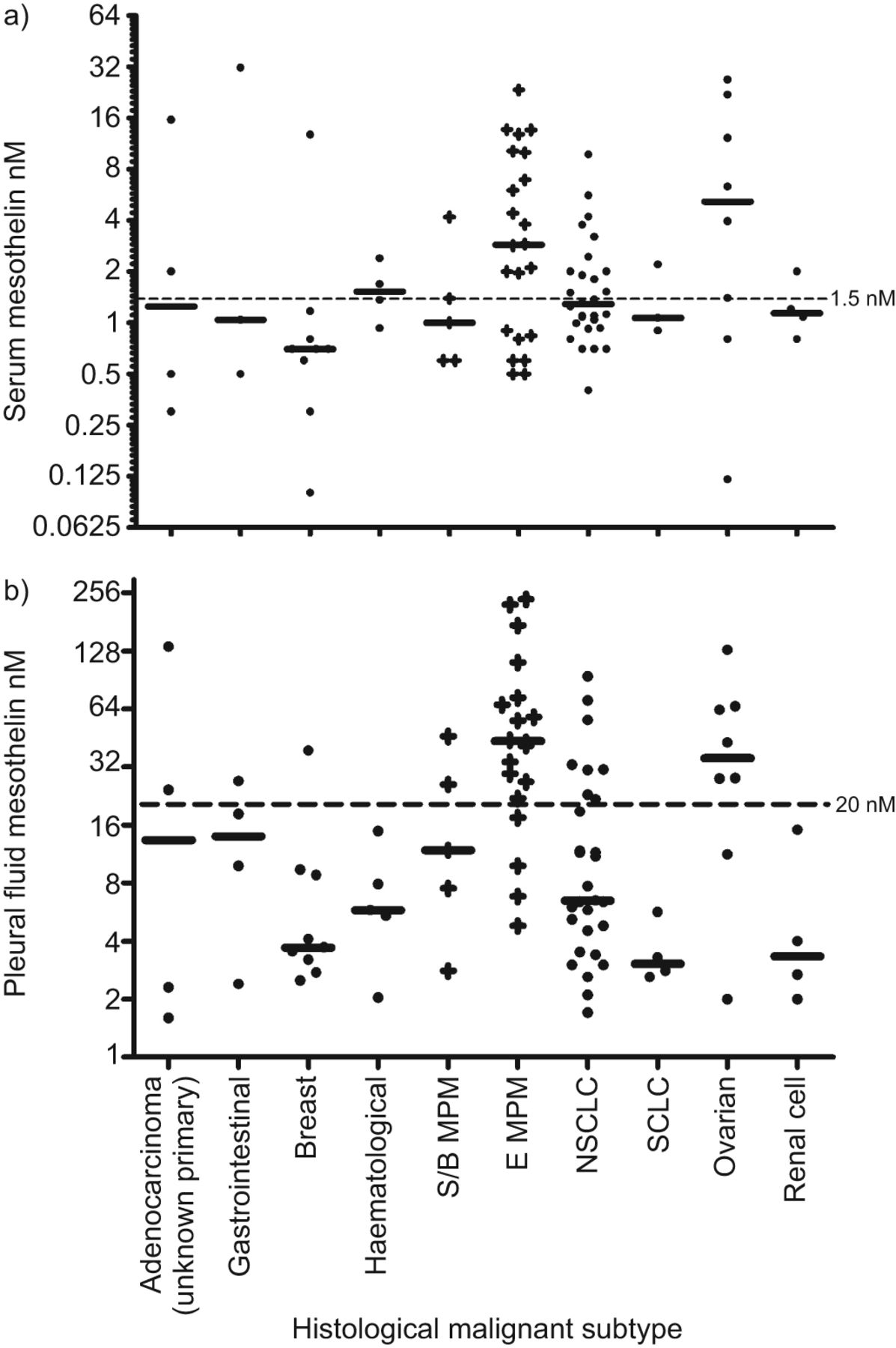
Positive serum mesothelin results were observed in 26 (38%) out of 69 patients and positive pleural fluid results in 19 (26%) out of 71 patients with non-MPM malignant pleural effusions, including those with adenocarcinoma of unknown primary, breast carcinoma, cholangiocarcinoma, chronic lymphocytic leukaemia, B-cell lymphoma, nonsmall cell lung cancer, ovarian carcinoma, primary peritoneal carcinoma, renal cell carcinoma and small cell lung cancer (fig. 2). A full breakdown of malignant histological sub-types is given in the online supplementary material.
{kind=link}
{kind=link}
a) Serum and b) pleural fluid mesothelin levels in histological sub-types of patients with malignant pleural effusions. Median levels in each group and positive cut-off level for mesothelin are shown. S/B MPM: sarcomatoid/biphasic malignant pleural mesothelioma; E MPM: epithelioid MPM; NSCLC: nonsmall cell lung cancer; SCLC: small cell lung cancer.
False-negative serum mesothelin was seen in three out of three patients with sarcomatoid MPM, one out of two biphasic MPM patients and seven out of 22 patients with epithelioid MPM, while a false-negative pleural fluid mesothelin was seen in three out of three sarcomatoid MPM and four out of 20 epithelioid MPM cases for whom samples were available.
Diagnostic characteristics of mesothelin for distinguishing MPM from other causes of pleural effusion
Excluding unconfirmed malignancy (radiographic diagnosis) and undiagnosed patients, serum mesothelin was examined in the group as a whole at a cut-off of 1.5 nM, yielding sensitivity 59.3% (95% CI 38.8–77.6%), specificity 64.7% (95% CI 57.2–72.0%), PPV 20.5% (95% CI 12.2–31.1%) and NPV 91.2% (95% CI 84.8–95.5%) (table 2).
Pleural fluid mesothelin was examined at a cut-off of 20 nM, giving sensitivity 72.0% (95% CI 50.6–87.9%), specificity 87.5% (95% CI 81.5–92.8%), PPV 46.2% (95% CI 30.1–62.8%), NPV 95.5% (95% CI 90.8–98.2%) (table 3).
Mesothelin testing within the investigation pathway for an undiagnosed pleural effusion
Data regarding the diagnostic accuracy of mesothelin testing in the context of cytology, CT scan and pleural biopsy results, and in patients with a final diagnosis of BAPE are given in the online supplementary material.
Comparative diagnostic accuracy of mesothelin measured in serum and pleural fluid
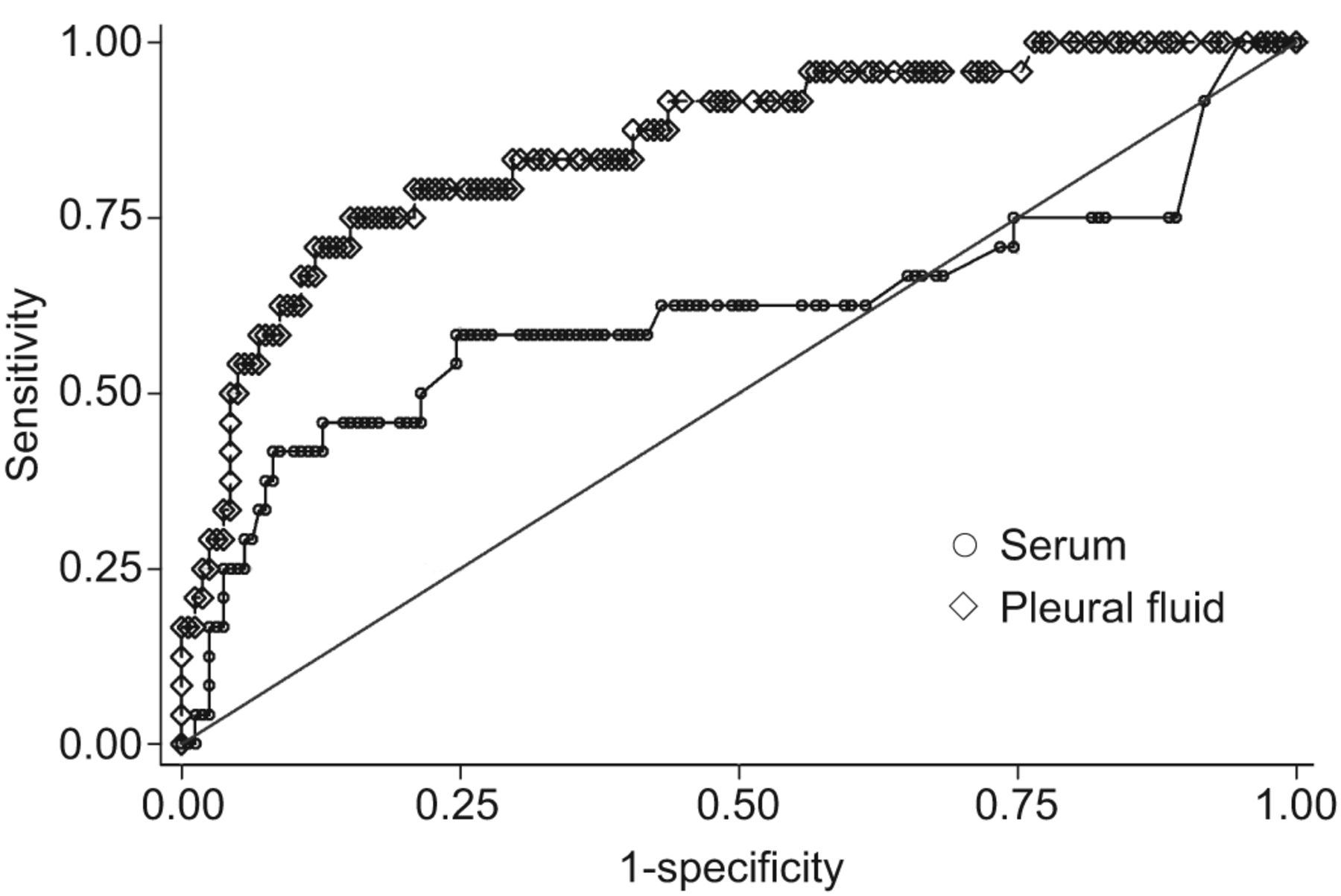
Considering only the 182 patients with a confirmed final diagnosis and both serum and pleural fluid mesothelin results (24 with MPM), the AUC for serum mesothelin in the diagnosis of mesothelioma was 0.61 (95% CI 0.46–0.77), which is significantly inferior to the AUC for pleural fluid at 0.85 (95% CI 0.77–0.94; p=0.0001) (fig. 3).
{kind=link}
{kind=link}
Receiver operating characteristics curves comparing the diagnostic accuracy of serum and pleural fluid mesothelin testing for the diagnosis of malignant pleural mesothelioma. Patients with both sample types and a definitive final diagnosis were included (n=182).
Diagnostic cut-off levels derived from both ROC curves at 95% specificity gave sensitivity 25.0% (95% CI 12.0–45.0%), PPV 46.0% (95% CI 23.0–71.0%) and NPV 89.0% (95% CI 84.0–93.0%) for serum (cut-off 0.975 nM), and sensitivity 50.0% (95% CI 31.0–69.0%), PPV 63.0% (95% CI 41.0–81.0%) and NPV 93.0% (95% CI 87.0–96.0%) for pleural fluid (cut-off 43.0 nM).
The impact of significant CKD
Contemporaneous creatinine and eGFR measurements were available for 229 out of 230 patients at the time of sample collection.
74 (32%) out of 229 patients had an eGFR ≤59 mL·min−1(stage 3 CKD or greater).
Specificity of serum mesothelin was 72.3% (95% CI 63.3–80.1%) in patients with an eGFR >59 mL·min−1but 49.1% (95% CI 35.6–62.7%) in those with eGFR ≤59 mL·min−1(tables 4and5). 19 (54%) out of 35 patients with a benign cause for pleural effusion but eGFR ≤59 mL·min−1had a false-positive serum mesothelin result.
Diagnostic characteristics of pleural fluid mesothelin were unaffected by renal function. Specificity with eGFR >59 mL·min−1was 86.0% (95% CI 78.2–91.8%) and with eGFR ≤59 mL·min−1, 87.0% (95% CI 75.1–94.6%).
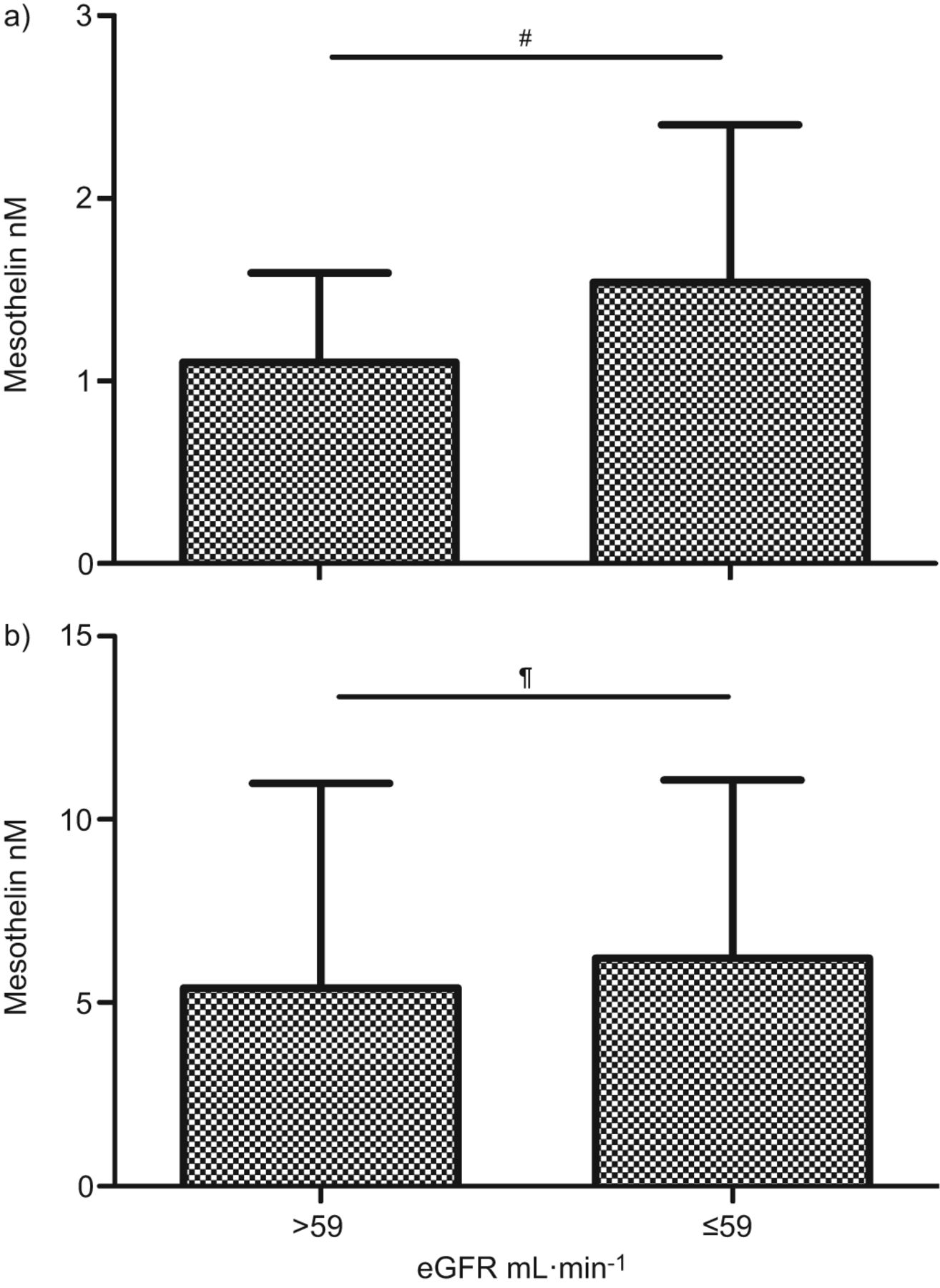
在我确认non-MPM诊断的患者,dian serum mesothelin was 1.54 (1.00–2.40) nM in patients with eGFR ≤59 mL·min−1, significantly higher than with an eGFR >59 mL·min−1at 1.1 (0.80–1.59) nM. Median pleural fluid mesothelin was not significantly different with (6.22 (3.0–11.07) nM) and without (5.41 (2.66–10.99) nM) renal impairment (fig. 4).
{kind=link}

{kind=link}
a) Serum and b) pleural fluid mesothelin in patients with a non-malignant pleural mesothelioma diagnosis with (estimated glomerular filtration rate (eGFR) ≤59 mL·min−1) and without (eGFR >59 mL·min−1) significant renal failure. Data are presented as median and interquartile range.#: p=0.007;¶: p=0.605.
There was no statistically significant association between age and serum or pleural fluid mesothelin when adjustment was made for the association between falling eGFR and increasing age.
DISCUSSION
This study has examined the practical application of mesothelin testing in serum and pleural fluid, in consecutive patients presenting with an undiagnosed pleural effusion.
Consistent with previous investigators, we have demonstrated significantly higher levels of mesothelin in serum and pleural fluid in patients with histologically confirmed mesothelioma than with pleural effusions of another cause, but a clinically important rate of false-positive results in patients with a wide range of non-MPM malignant sub-types as well as benign disease [8,9,13–17]。
Mesothelin is expressed on normal mesothelium [18] and gene expression studies confirm overexpression on malignant cells of many histological sub-types including MPM, ovarian, pancreatic, endometrial, lung, oesophageal, colonic, vulval and cervical malignancies [19]。Lack of specificity amongst non-MPM malignant pleural effusions is therefore explicable and well documented, but does represent a substantial limitation to the clinical utility of the test.
False-positive serum results in patients with benign diagnoses were also very common in our series; 36 (34%) out of 107 patients with a benign diagnosis had a positive serum mesothelin at a cut-off level of 1.5 nM. Pleural fluid mesothelin was positive in only two patients with benign disease; both had a final diagnosis of robustly ascertained BAPE.
患者的积极成果安逸猿也een commonly with the serum test (five out of 13 patients). All patients had a lack of radiographic progression on serial CT scan for at least 12 months and all but one had irrefutable histological confirmation of benign disease.
Immuno-histochemical studies have shown that most sarcomatoid sub-type MPM tissue does not express mesothelin, such that the “false” negative test results shown in this and previous studies are to be expected [20]。Serum and pleural fluid mesothelin were also negative in 32% and 20% of patients with epithelioid sub-type disease, presumably reflecting variable gene expression.
We have demonstrated superior diagnostic characteristics for pleural fluid mesothelin above serum within paired results alone, at a fixed specificity of 95%, and using established cut-off levels, at each stage in the diagnostic pathway. This contrasts with the conclusion of several earlier series examining smaller numbers of paired results that have not demonstrated a significant difference between pleural fluid and serum analysis [8,13]。
Overall the NPV of mesothelin when measured in serum (91.2%) and pleural fluid (95.5%) is good, but the PPV (20.5% and 46.2%, respectively) is not within a clinically useful range.
A recent study by Boudvilleet al.[10] examined serum mesothelin levels in 144 patients with stable CKD but no clinically apparent pleural disease and demonstrated significantly higher levels in patients with CKD stage 3 or greater compared to those with CKD stage 2, suggesting that mesothelin, released from normal mesothelial cells, undergoes a degree of renal clearance, consistent with its small molecular mass. Hollevoetet al.[11] measured serum mesothelin and glomerular filtration rate (GFR) in 66 control patients, demonstrating a positive correlation between GFR and the reciprocal of serum mesothelin and a false-positive rate of 52% in patients with CKD stage 3 or greater.
在our series, specificity of serum mesothelin was 72.3% in patients with an eGFR >59 mL·min−1在CKD患者,相比之下,49.1%阶段3or greater. 20 out of 36 positive serum tests in patients with benign pleural effusions may be explained by significant renal failure. Levels of mesothelin measurable in pleural fluid in patients without mesothelioma were not affected by renal function and the diagnostic accuracy of the test when applied to pleural fluid was not significantly different between the two renal function groups. While accumulation of mesothelin in pleural fluid as a result of diminishing renal clearance would not necessarily be expected (as it would in serum), this is the first study to demonstrate this potential advantage of pleural fluid testing.
There are several notable limitations to this study. While it is one of the largest reported series of patients presenting with pleural effusions to undergo mesothelin testing, the proportion of patients with mesothelioma was low when compared with most previous studies that have selected samples from established tissue banks by diagnosis. However, this proportion accurately reflects our consecutive patient population. We studied the diagnostic accuracy of mesothelin at previously established cut-off levels, which, while achieving the study aim (to examine the test in a clinically relevant manner), may produce inferior diagnostic characteristics than derivation of cut-off levels specific to our patient population or according to a desired sensitivity or specificity. Finally, conclusions regarding the utility of the test when applied to pleural fluid are tempered by the current lack of validation of commercially available ELISAs for this sample type.
本研究的力量的招聘n unselected consecutive series of patients with pleural effusions requiring investigation and the robust application of diagnostic criteria, diagnosis of MPM exclusively on histological grounds and patient follow-up to 12 months in the presence of benign pleural disease. Within this complex “real world” sample, the specificity and PPV of mesothelin are challenged.
在conclusion, these results suggest that the routine testing of mesothelin in all undiagnosed pleural effusions is unhelpful. If the test is performed for diagnostic purposes, pleural fluid should be used instead of serum, particularly in patients with an eGFR ≤59 mL·min−1. A negative result in a patient with a low pre-test probability of MPM is reassuring for an absence of epithelioid mesothelioma and NPV appears to be relatively consistent between serum and pleural fluid. Positive test results, however, should be interpreted with caution, as false positives are common, including in patients with BAPE. The role of the test in MPM diagnosis therefore appears limited. Serum mesothelin has shown promise in monitoring treatment response and disease progression [21–24] and this should be the focus of future studies.
Acknowledgments
The authors would like to acknowledge M. Darby and I. Laurence (Dept of Radiology, North Bristol NHS Trust, Bristol, UK) for their assistance with radiological aspects of the study, N. Ibrahim and M. Brett (Dept of Histopathology, North Bristol NHS Trust) for their histology and cytology contributions and K. Elvers (University of Bristol, Bristol) for assisting with mesothelin assays. Mesomark® test kits were provided at reduced cost by Fujirebio Diagnostics Inc. (Malvern, PA, USA).
Footnotes
This article has supplementary material available fromwww.www.qdcxjkg.com
Clinical Trial
This study is registered at UK Clinical Research Network with adoption number 8960.
Statement of Interest
Statements of interest for J.E. Harvey and N.A. Maskell, and for the study itself can be found atwww.www.qdcxjkg.com/site/misc/statements.xhtml
- ReceivedAugust 26, 2011.
- AcceptedApril 2, 2012.
- ©ERS 2013
REFERENCES










