





数据
-
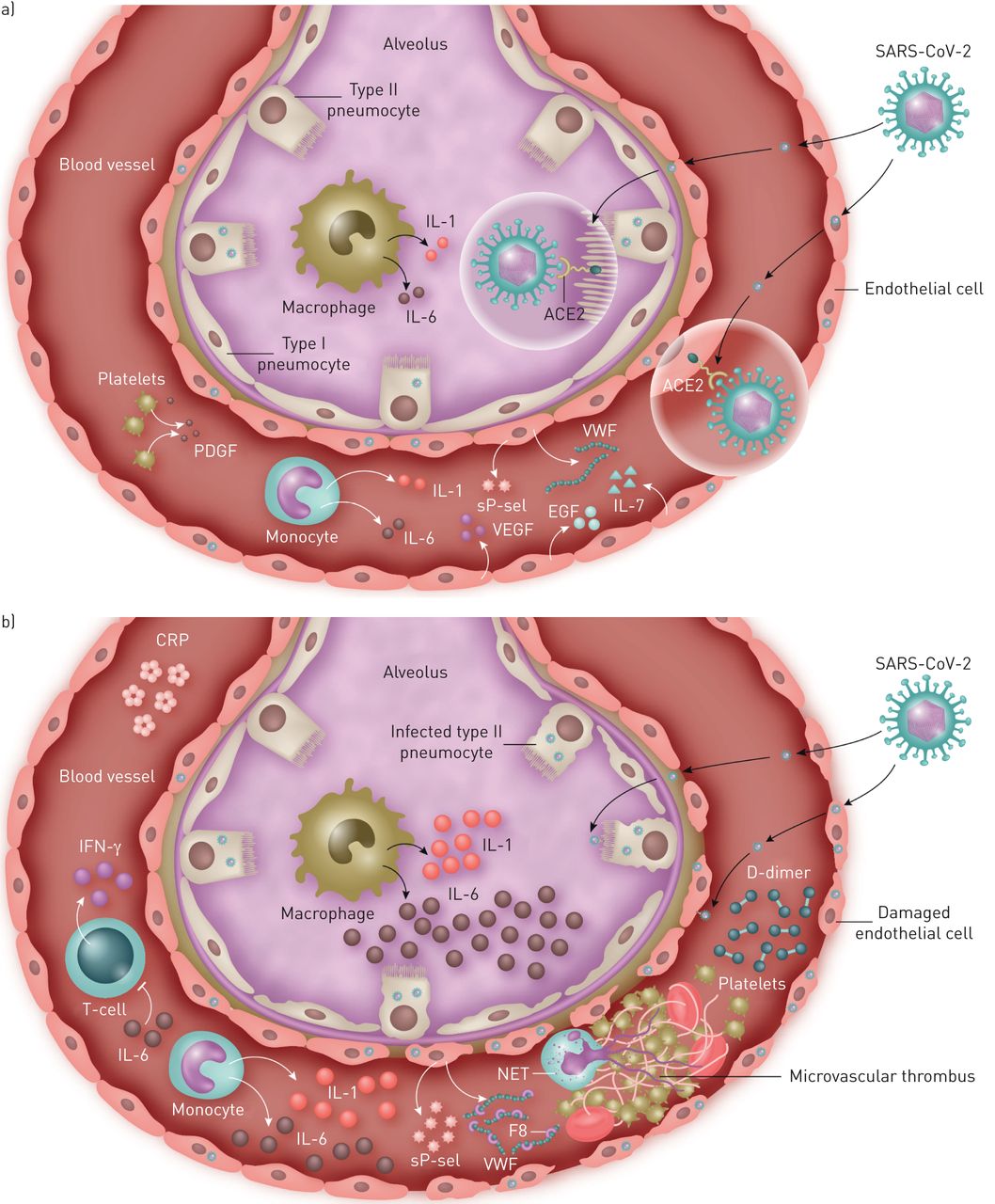
图1
新型严重急性呼吸综合征冠状病毒2 (SARS-CoV-2)在一些患者中引起轻微疾病,在另一些患者中引起严重疾病的机制示意图。在这两种情况下,病毒都进入人体细胞通过与血管紧张素转换酶2 (ACE2)结合,ACE2是一种在II型肺细胞、巨噬细胞、内皮细胞和其他肺细胞中广泛表达的跨膜受体[24,25].a)病情轻(凝血和血栓发生率低,住院时间短,危重症和病死率低):这类患者血清炎症因子低,组织修复性生长因子如表皮生长因子(EGF)、血小板衍生生长因子(PDGF)、白细胞介素(IL)-7等较高[5].VEGF:血管内皮生长因子。b)重症(大、微血管血栓发生率高,住院时间长,危重症高,病死率高):多为细胞因子风暴,血清炎性细胞因子(如IL-6、IL-1、IFN-γ)较高,内皮激活标志物如血管性血友病因子(vWF)、8型凝血因子(F8)、可溶性p -选择素(sP-sel)等,导致内皮炎和微血管血栓形成[5,15,27].IL-6显著升高导致淋巴细胞减少和免疫瘫痪,IL-6阻断可部分恢复[4,32].NET:中性粒细胞细胞外陷阱;CRP: c反应蛋白。
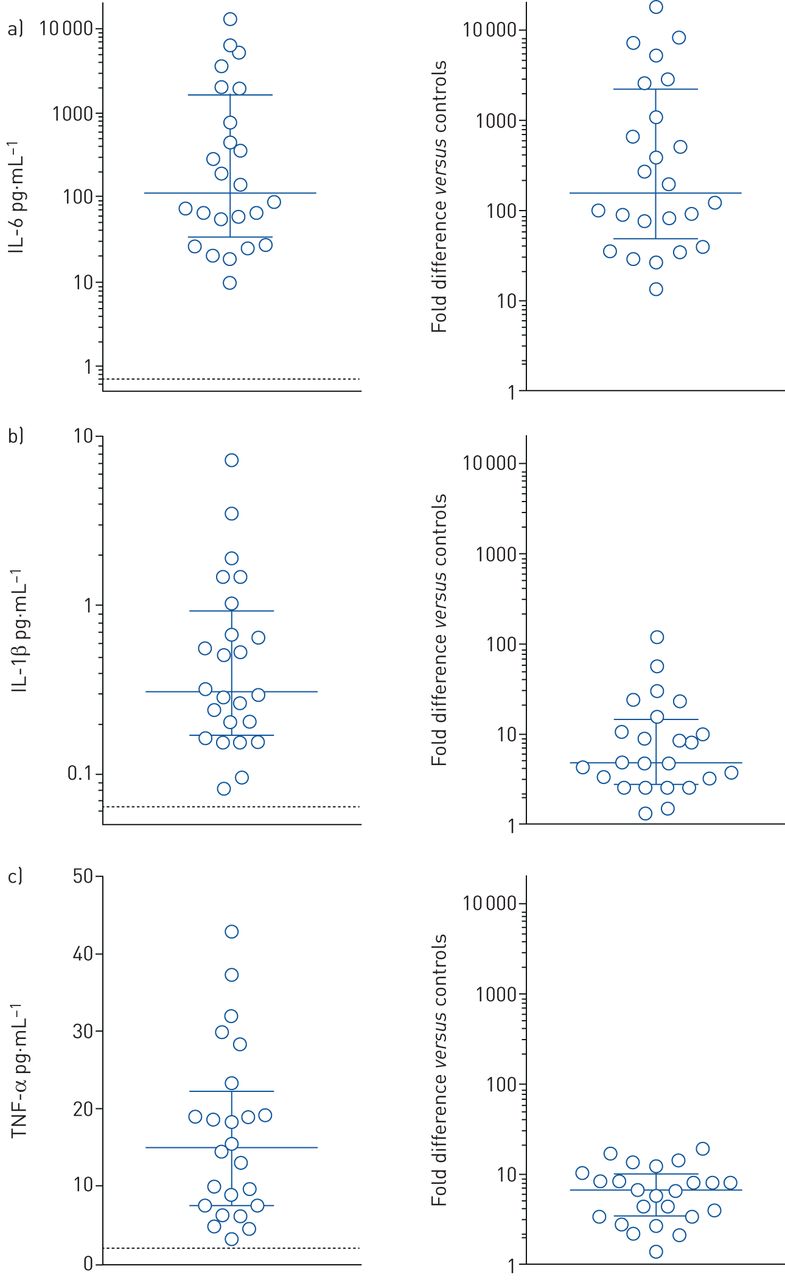
细胞因子的绝对水平及其与标准值相比的升高。描述的是来自24名2019冠状病毒病(COVID-19)重症患者温哥华队列的a)白介素(IL)-6, b) IL-1β和c)肿瘤坏死因子(TNF)-α的峰值水平。此外,我们已经表示了在COVID-19患者和健康对照组中观察到的细胞因子水平之间的相应倍数差异(即。右侧为每个细胞因子的规范值)。这些标准值可以被视为IL-6的水平虚线(值0.71 pg·mL)−1), IL-1β(值0.064 pg·mL−1)和TNF-α(值2.23 pg·mL−1).所有数值均来自Simoa HD-1分析仪[13,33].











![Schematic representation of mechanisms by which the novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) causes mild disease in some patients and severe disease in others. In both cases, the virus enters human cells via binding to angiotensin-converting enzyme 2 (ACE2), a transmembrane receptor widely expressed in type II pneumocytes, macrophages, endothelial and other pulmonary cells [24, 25]. a) Mild disease (low incidence of coagulopathy and thrombosis, shorter hospital stay, low critical illness and mortality): these patients have low serum inflammatory cytokines and high tissue reparative growth factors such as epidermal growth factor (EGF), platelet derived growth factor (PDGF), and interleukin (IL)-7 [5]. VEGF: vascular endothelial growth factor. b) Severe disease (high incidence of micro- and macrovascular thrombosis, longer hospital stay, high critical illness, and mortality): many of these patients have cytokine storm, with high serum inflammatory cytokines (such as IL-6, IL-1, IFN-γ) and markers of endothelial activation such as von Willebrand factor (vWF), factor 8 coagulant (F8) and soluble P-selectin (sP-sel), resulting in endothelialitis and microvascular thrombosis [5, 15, 27]. Markedly elevated IL-6 leads to lymphopenia and immunoparalysis which is partially restored by IL-6 blockade [4, 32]. NET: neutrophil extracellular trap; CRP: C-reactive protein.](http://www.qdcxjkg.com/content/erj/56/4/2003006/F1.large.jpg?width=800&height=600&carousel=1){kind=link}
{kind=link}
![Absolute cytokine levels and their elevation compared to normative values. Depicted are the peak levels for a) interleukin (IL)-6, b) IL-1β and c) tumour necrosis factor (TNF)-α from a Vancouver cohort of 24 critically ill coronavirus disease 2019 (COVID-19) patients. Further, we have represented the corresponding fold difference between cytokine levels observed in the COVID-19 patients and those of healthy controls (i.e. normative values) on the right-sided figure for each cytokine. These normative values can be seen as a horizontal dashed line for IL-6 (value 0.71 pg·mL−1), IL-1β (value 0.064 pg·mL−1) and TNF-α (value 2.23 pg·mL−1). All values were derived from the Simoa HD-1 analyser [13, 33].](http://www.qdcxjkg.com/content/erj/56/4/2003006/F2.large.jpg?width=800&height=600&carousel=1){kind=link}
{kind=link}