





一种bstract
儿童在线哮喘管理可以(部分)替代常规门诊访问,并且具有成本效益http:///wly/oabk30f7sre.
到编辑:
提出了电子健康干预措施作为一个应用程序ealing method to improve health outcomes and reduce healthcare costs [1-3.]。但是,eHEPHEATH干预的发展与高成本有关,这种投资需要通过增加的临床效果和相关成本节约来平衡。不幸的是,母羊健康有效性方面的稳健证据仍然有限[2-5.], as is evidence regarding cost-effectiveness. This causes uncertainty about the effectiveness of eHealth and constitutes a barrier towards successful implementation in daily practice [6.那7.]。因此,有必要评估效果和成本效益,以说服其附加值的同事和政策制定者。
W.e assessed the cost-effectiveness of online asthma care for children alongside a randomised controlled trial (RCT) to evaluate the effectiveness of this eHealth intervention on health improvement [8.]。一世n this RCT, 210 asthmatic children were randomly allocated into two groups of asthma management. In the usual care (UC) group, care consisted of routine 4-monthly outpatient visits where asthma control was assessed with an asthma control test (ACT)/children's asthma control test (C-ACT) [9.]。一种lternatively, in the virtual asthma clinic (VAC) group, outpatient visits were reduced by 50% and asthma control was monitored online with monthly web-based ACT/C-ACT tests. In the VAC group, children had more symptom-free days per month and their ACT/C-ACT scores were more improved. As such, this RCT proved that routine outpatient visits can partly be replaced by online asthma management using the VAC.
W.e carried out an先验defined cost-effectiveness analysis with the hypothesis that online management通过VAC具有成本效益。标准成本问卷由父母完成每4个月,以评估医疗保健和社会角度的成本。医疗保健(或直接)成本包括与医疗条件相关的所有费用,规定的药物和干预费用(包括VAC和估计托管和许可费用)。社会(或间接)成本包括生产力损失,任何医疗条件和停车费的旅行费用。成本基于荷兰成本分析指南[10.虽然如果使用价格没有其他来源。使用荷兰消费者价格指数,价格被转换为2014年级别[11.]。
在哮喘相关的寿命(QOL)和哮喘控制方面,平均增量成本对平均增量效应进行加权。增量成本效益比(ICER)的不确定性边界(ICER)使用自举分析确定。在此自动启动仿真中,使用替换选择1000个成本效果对的样本。模拟结果以图形方式呈现在散点图中,其中每个点表示引导刺激的一次迭代的转换器。两个经过验证的问卷均用于评估0,8和16个月的QOL:儿科哮喘护理人员的生活质量问卷(PACQLQ)评估幼儿的护理人员(6-12岁)和儿科哮喘质量的生活问卷调查问卷(PAQLQ)为青少年(12-16岁)[12.那13.]。通过用于RCT所述的ACT / C-Act测量哮喘控制。使用非参数曼诺 - 惠特尼U-Test评估成本的差异。使用线性混合模型分析了ACT / C-ACT和PACQLQ / PAQLQ中基线的变化。
16个月后,幼儿哮喘控制(C-ACT)在VAC组中较高,平均值(95%CI)差为1.17(0.09-2.25)点(P = 0.03)[8.]。一世n the group of teenagers, no significant difference in ACT score between treatment arms was observed with a mean (95% CI) difference of 0.88 (−0.41–2.16) points. In addition, a 50% reduction in the number of outpatient visits did not have any relevant influence on PACQLQ and PAQLQ results (data not presented; p=0.95 and 0.84, respectively).
VAC组每位患者的直接和间接成本明显低于UC集团(中位VAC€726.52 /中位UC€875.86(P = 0.01)和中位VAC€102.79 /中位UC€124.56(P = 0.02),分别)。与UC相比,这导致了VAC的社会观点(直接加上间接成本)的总成本较低(中位VAC€889.77 /中位UC€1081.47(P = 0.014))。以下医疗保健和社会成本没有显着差异:GP咨询,儿科医生咨询,其他专家,物理治疗师,通过电话,急诊室访问,医院入学和生产力丧失(未提出的数据)。在线哮喘管理与较低的成本有关,因为门诊诊所访问较少(中位VAC€237.09 /中位UC€385.15(P <0.000))和较低的旅行费用(中位VAC€94.09 /中位UC€120.15(P = 0.003))。
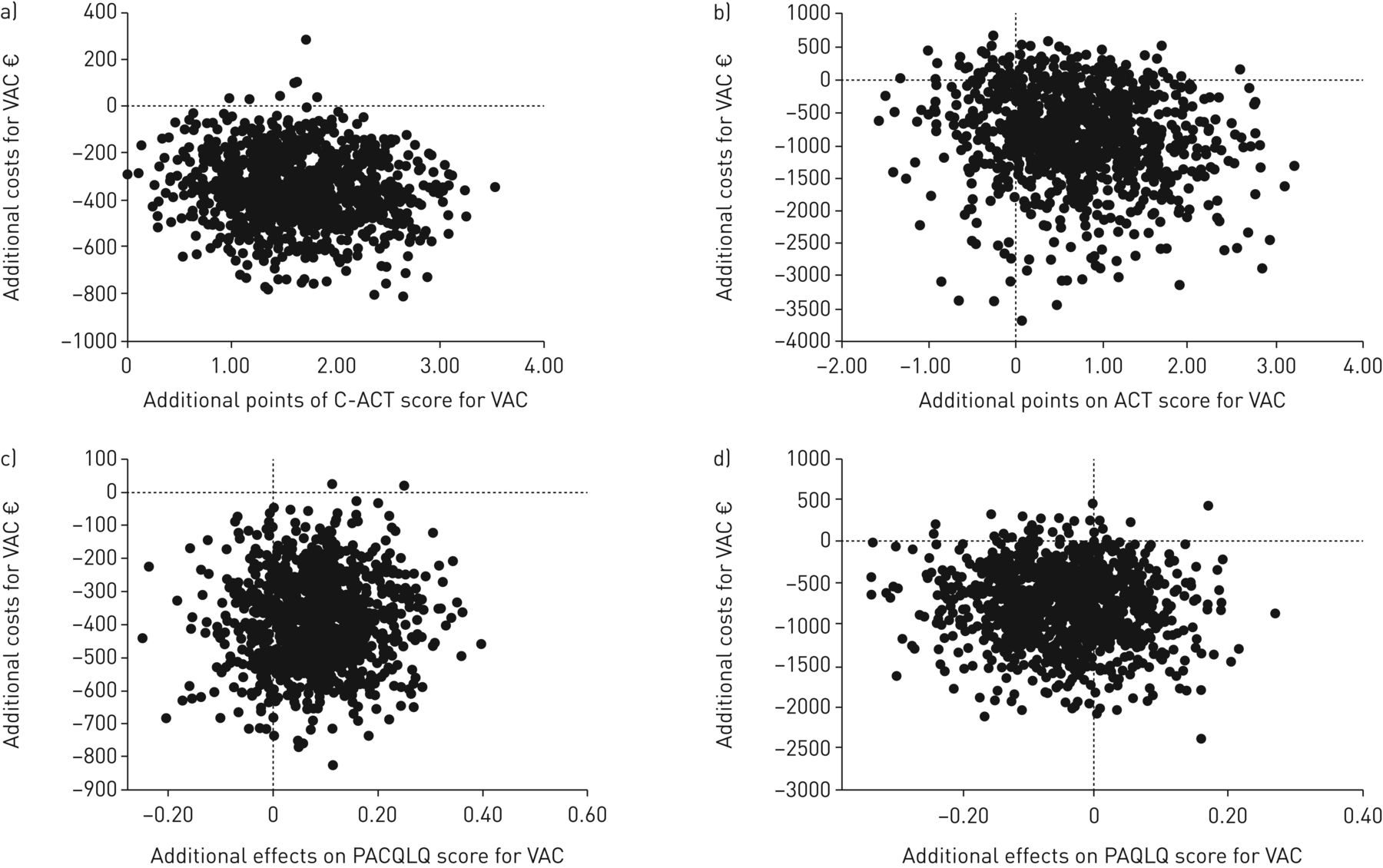
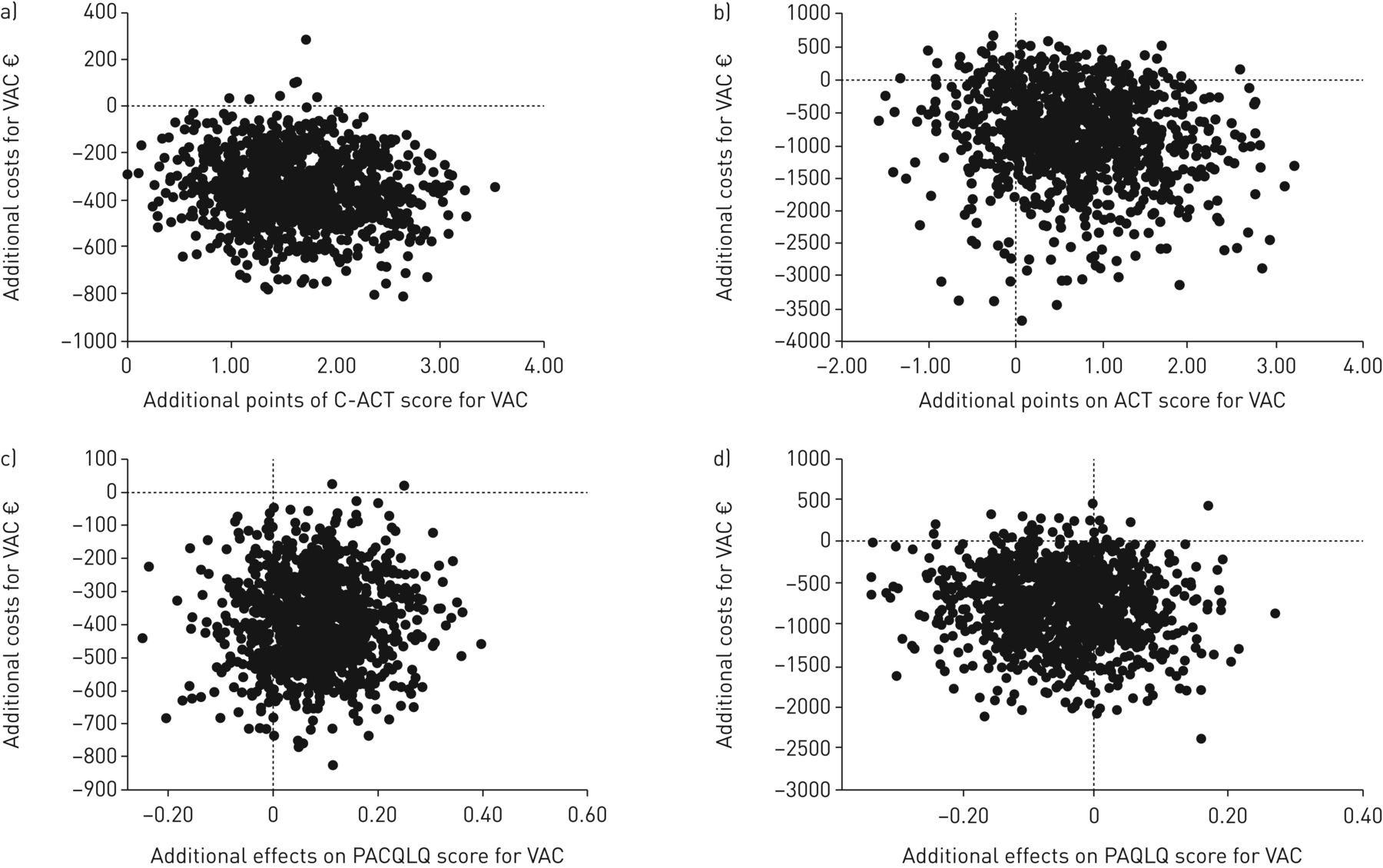
在幼儿中,VAC导致了1000个抢夺重复的99%的健康结果和成本节省,每位患者的平均成本为352欧元(第95百分位数:67欧元和652欧元)(图1A)。在青少年中,在90%的抢夺重复中实现了相当大的成本节省,平均节省了每位患者852欧元(95百分位数:€-294和2584欧元)(图1B.)。两组哮喘控制相似,造成的搬运复制百分比,导致改善的健康结果和成本节约为74%。关于QOL和成本的成本效益飞机(图1C.和1 d)。生命质量是维护而节约成本ere realised for online care in both age groups.
Cost-effectiveness planes showing the cost-effectiveness of a virtual asthma clinic (VAC) compared with usual care (1000 bootstrapped estimates). Dots represent the societal costs (direct plus indirect costs) plotted against asthma control for a) young children (6–11 years; asthma control measured by C-ACT) and b) teenagers (12–16 years; asthma control measured by ACT) or against quality of life for c) caregivers of young children (quality of life measured by PACQLQ) and d) teenagers (quality of life measured by PAQLQ). The South-East quadrants in a, b, and c indicate that the VAC dominates usual care (即有效性更高,成本较低);但是,D中的较低象限表明,虽然成本较低,有效性是相同的。C-CAR:儿童哮喘控制测试;作用:哮喘控制测试;PACQLQ:儿科哮喘护理人员的生活质量问卷;PAQLQ:儿科哮喘质量的生活问卷。
总之,我们展示了与UC相比,常规门诊次数减少50%的儿童的在线哮喘管理的成本效益。在幼儿中,在线护理导致改善的健康结果和大量的成本节约。在青少年,UC和网上护理对临床结果同样有效,但在线护理实现了相当大的成本节省。这种成本效益分析支持从健康经济学的角度实施在线哮喘管理。虽然有关电子医疗临床效率的证据积累,但其成本效益的证据仍然是稀缺[3.那14.]。对电子医疗经济评估的主要局限性是缺乏RCT和缺乏质量数据和适当措施[14.那15.]。此外,除了我们的研究表格外,大多数电子健康干预措施除了我们的学习,还使用了eHealth部分取代UC的研究。国家航空航空公司的国家实施有可能在每年1070万欧元(包括直接和间接费用)的成本,基于荷兰的儿科医生治疗的哮喘患者,达到每年1070万欧元(包括直接和间接成本)。在其他国家的在线儿科哮喘护理可能会降低成本的成本,特别是当医疗费用较高或旅行距离更大时。人们可以争辩说,现实生活中的常规访问的频率与RCT中的固定协议不同,并且一些患者应更频繁地看到患者。对个体患者的一般方法是不可取的,医疗保健的重点是从交付的服务量转移到增加患者价值。与医生的需求一致,对个人患者的愿望定制保健至关重要。这是VAC的优势之一:它反映了“个性化eHealth”的发展。此外,它是基于价值的医疗保健的一个很好的例子:为患者提供适应个人的患者的高价值,同时通过更换更频繁的在线监测来降低不常见的传统门诊访问来降低成本,这既比效率更有效,更耐心。
W.e conclude that the VAC for children is an effective and cost-effective eHealth intervention to improve asthma care. Introducing this intervention as part of current asthma management is an attractive and very realistic option to optimise monitoring strategies in a more personalised way. The next step is implementation and routine use of this intervention in daily practice.
D.isclosures
S.upplementary Material
L.S.van den wijngaart.ERJ-01413-2017_VAN_DEN_WIJNGAART.
致谢
一种uthor roles:Merkus.那Peter; Pijnenburg, Mariëlle; Verhaak, Chris designed the study and obtained funding. van den Wijngaart, Lara; Roukema, Jolt; Boehmer, Annemie; Brouwer, Marianne; Verhaak, Chris; Niers, Laetitia; Sprij, Arwen; Rikkers-Mutsaerts, Eleonora; Rottier, Bart; Pijnenburg, Mariëlle; Merkus, Peter all participated as investigators, recruited patients and performed treatments. van den Wijngaart, Lara carried out the analyses. Kievit, Wietske conducted the cost-effectiveness analysis. van den Wijngaart, Lara; Kievit, Wietske; Roukema, Jolt; Merkus, Peter operated as the writing committee and drafted the manuscript until it reached its final form. All authors commented on the manuscript and its revisions. Merkus, Peter is the guarantor of the study.Ethical approval:这项研究由所有当地伦理委员会批准。所有参与者都提供了书面知情同意书。数据共享:患者级数据可以从相应作者的合理要求提供。未获得患者同意,但呈现的数据是匿名的,并且缺少识别风险。Transparency declaration:牵头作者肯定了本手稿是诚实,准确和透明的研究报告的陈述,即没有省略该研究的重要方面,并且根据计划(以及相关,注册)的研究中的任何差异已经解释过。事先演示:在欧洲呼吸协会(Amsterdam,2015)的大会上提出了这种随机对照试验的结果。188bet官网地址国际儿科肺部大会上提出了成本效益分析的结果(那不勒斯,2016年)。谢谢:我们感谢所有参与的儿童和父母为他们对本研究的贡献,以及合作的儿科医生和Sintnicolaas,Coosje(Radboud University Center,Amalia Childer的医院,儿科肺部,Nijmegen,Netherlands);佩特拉史蒂文斯(佩戴尔威廉纳医院,假日部,尼斯特纳,荷兰);Verwaal,Mariël(Maasstad医院,儿科,罗特丹,荷兰);大胆的,卡罗拉(Maxima Medical Center,Paediatrics系,Veldhoven,荷兰);冬季,ANS(莱顿大学医学中心,儿科肺部,莱顿,荷兰);Mulder,Ineke和Van Baak,Christine(朱氏医院,Juliana儿童医院,小儿科肺部,海牙,荷兰);Spiersings,Magda和Hiddinga,Jantine(伊拉斯族医学中心,索菲亚儿童医院和Kinderhaven / Havenziekenhuis,儿科肺部,荷兰鹿特丹)为他们的热情和他们在招募和监测患者的努力。W.e acknowledge Hop, Wim (Erasmus Medical Centre, Department of Biostatistics, Rotterdam, The Netherlands) and Moll, Henriëtte (Erasmus Medical Centre, Sophia Children’s Hospital, Department of Paediatrics, Rotterdam, The Netherlands) for performing the interim safety analysis and also commemorate van Gent, Rene (Maxima Medical Centre, Department of Paediatrics, Veldhoven, The Netherlands) and thank him for his contributions to this study.
Footnotes
支持声明:本研究由荷兰肺基金会资助(Grant:3.4.10.016)和荷兰健康保险公司的创新基金(Grant:B 10-135)。资助者在试验设计,数据收集,分析或报告中没有作用。本文的资金信息已存入Crossref Funder Registry。
利益冲突:可以在本文中找到披露www.qdcxjkg.com
- 收到2017年7月13日。
- 公认july 23, 2017.
- 版权所有©2017











{kind=link}
{kind=link}