





抽象
门肺高压(POPH)被认为是肺动脉高血压(PAH)亚型;然而,建立PAH的治疗目前尚未评估此条件。
The current authors treated 14 patients (four male, 10 female; mean (range) age 55 (39–75) yrs) with moderate (n = 1) or severe (n = 13) POPH caused by alcoholic liver disease (n = 7), chronic viral hepatitis (n = 3), autoimmune hepatitis (n = 3), and hepatic manifestation of hereditary haemorrhagic teleangiectasia (n = 1) with oral sildenafil. Eight patients were newly started on pulmonary vasoactive treatment, while six patients were already on treatment with inhaled prostanoids (iloprost, n = 5; treprostinil, n = 1). During treatment with sildenafil, mean±SD6-min walk distance increased from 312±111 m to 397±99 m after 3 months, and 407±97 m after 12 months. Mean±SDpro-brain natriuretic peptide levels decreased from 582±315 ng·mL-1to 230±278 ng·mL-1,和189±274ng·mL的-1after 3 and 12 months, respectively. Two patients died after 1 and 2 months from liver failure and cardiac failure, respectively. There was a similar response to sildenafil treatment after 3 and 12 months in patients on monotherapy and those on combination therapy.
In conclusion, sildenafil might be effective in monotherapy and in combination therapy with inhaled prostanoids in portopulmonary hypertension, leading to significant improvement by 3 months and sustained response over 12 months.
肝病患者是在开发肺血管并发症的风险1。其中,门肺高压(POPH)是影响肝硬化患者2-10%,罕见但严重的并发症。它与死亡率增加有关,由于阻塞性肺血管病变和有肝脏疾病潜在的治疗方案产生重大影响2。POPH的发展一直与门静脉高压,但它可以发生在肝脏疾病的任何阶段,随着发病率越来越依赖于肝损害的严重程度3。患者POPH是在肝移植过程中出现严重并发症的高危人群4。
POPH被视为肺动脉高血压亚型(PAH)五。然而,对于PAH新开发的治疗策略一直没有研究,也没有批准POPH。此外,POPH已明确从PAH最近发表的随机对照试验排除6。
目前肺血管活性治疗提供化合物已经在POPH已经成功地使用,甚至能够成功肝移植7,8。到目前为止,病例报告和病例系列已经出版显示静脉注射和吸入前列腺素,口服波生坦或联合用药治疗临床,功能和血流动力学的好处9-13。
磷酸二酯酶5抑制剂西地那非目前许可用于PAH的治疗。它拥有的是与肺vasoselective行动,但没有肝毒性的口服复方优势14。在POPH成功使用西地那非的最近报道两个案例研究15,16。
当前作者评估长期治疗西地那非的POPH,主要目标是安全性和有效性任一单一疗法或与吸入前列腺素组合。
患者和方法
在当前的作者的三级转诊中心肺血管疾病,与PAH与肝脏疾病有关的所有患者进行了评价,以确定:1)肝硬化和肝癌疾病的根本病因的程度;2)症状根据世界卫生组织(WHO)的分类有关PAH;使用6分钟步行距离(6- MWD)根据美国胸科协会准则3)运动能力17;4)使用权,心脏血流动力学导尿参数。
Pulmonary vasoactive treatment was started when patients were in WHO functional stage III–IV, with an impaired exercise tolerance and moderate-to-severe pre-capillary pulmonary hypertension with increase of mean pulmonary arterial pressure (mPAP) >35 mmHg1,and a pulmonary vascular resistance (PVR) >500 dyne·s·cm-518。
的患者在本研究中没有正在与β阻断剂治疗。Patients on prostanoid treatment received either iloprost 6 inhalations·day-1with a total daily dose of 30 µg (n = 5), or treprostinil 4 inhalations·day-1with a total daily dose of 120 µg (n = 1) at mouthpiece using an ultrasonic inhalation device. Sildenafil treatment was started with increasing dosage, reaching 50 mg three times daily within 3 weeks in all patients. Follow-up included: clinical assessment; measurement of 6-MWD; laboratory studies including liver function tests and pro-brain natriuretic peptide (pro-BNP) measurement; and right-heart catheterisation after 3 months and 12 months.
由于数据是正态分布的,结果显示为平均值±SD。为了检测组之间的统计学差异显著,双面,使用非配对t-检验。对于治疗效果的评估,双面,使用配对t检验。For subgroup analysis, ANOVA (α = 0.05) and事后分析被应用。用于多重比较的校正Bonferroni校正19。
结果
其中32例POPH,20名晚期患者(即根据最近的指导疾病的中度或重度阶段1)进行了鉴定。Øf these, 12 patients were already receiving therapy with inhaled iloprost (n = 7), inhaled treprostinil (n = 2) or endothelin-receptor blockers (n = 3). Sildenafil treatment was considered in newly diagnosed patients and in patients not stable on current therapy. Six patients were stable on treatment with endothelin-receptor blockers (n = 3) or inhaled prostanoids (iloprost, n = 2; treprostinil, n = 1) and were not included in the study.
Sildenafil treatment was started in 13 patients with severe and one patient with moderate POPH but in WHO functional class III (four male, 10 female; mean age 55±12 yrs). Six patients had already been on active treatment with inhaled prostanoids (iloprost, n = 5; treprostinil, n = 1) for mean (range) 20 (3–42) months, but required additional treatment. Underlying aetiologies included liver cirrhosis caused by alcohol liver disease (n = 7), or associated with viral hepatitis (n = 3), autoimmune hepatic diseases (n = 3) or hepatic involvement in hereditary haemorrhagic teleangiectasia (HHT; n = 1). Patients were in either clinical stage Child A (n = 7), B (n = 6) or C (n = 1).
Concerning pulmonary hypertension, patients were in WHO functional classes III (n = 10) and IV (n = 4) with a mean 6-MWD at baseline of 307±109 m.
Pre-capillary pulmonary hypertension was confirmed on right-heart catheterisation with mPAP 55±11 mmHg, cardiac index of 2.2±0.8 L·min-1·米-2and PVR of 1130±688 dyne·s·cm-5。Øne patient (patient 5) in WHO class III with mPAP 59 mmHg and PVR 438 dyne·s·cm-5也包括在研究中。
Within 3 months of treatment beginning, two patients had died. The patient with hepatic involvement of HHT (patient No. 13) was already in an advanced stage of liver cirrhosis when referred for assessment of POPH. The patient died in progressive liver failure 1 month after the start of sildenafil therapy. There were no additional causes of liver disorder. Notably, there were no signs of a bleeding event.
患者编号14,与病毒性肝硬化,在吸入的伊洛前列素治疗初步改善相关的严重POPH;然而,她需要与西地那非由于病情发展联合治疗。The patient died in cardiac failure 2 months after starting combination therapy. Again, there were no signs of a bleeding event.
The other 12 patients completed 3 months’ follow-up, with an increase in 6-MWD from 312±111 m to 397±99 m (p = 0.001). There was a significant decrease in mPAP, from 55±11 mmHg to 46±10 mmHg (p = 0.01), an increase in cardiac index from 2.2±0,8 L·min-1to 2.8±1.0 L·min-1(p = 0.06), and a significant decrease in PVR from 1,070±597 dynes·s·cm-5to 698±358 dyne·s·cm-5(p<0.05; table 1⇓)。Pro-BNP levels decreased from 582±315 ng·mL-1to 230±278 ng·mL-1(p = 0.06). Liver function test, arterial partial pressure of oxygen (PØ2) and haemoglobin levels remained stable (table 2⇓)。
讨论
POPH包括PAH的不同病因。但是,它并没有在最近的随机对照试验研究了用于治疗肺动脉高压6,14。因此,POPH的治疗依赖于同情使用目前可用于治疗PAH化合物。在此患者人群的有效性和肺血管活性治疗的安全可用的资料很少。In the current retrospective study, a significant clinical, functional and haemodynamic improvement was found over 3 months’ treatment with oral sildenafil in patients with severe POPH. Successful treatment of POPH has been reported using prostanoids or endothelin-receptor antagonists, with observation times of 3–12 months9-13。皮下,静脉注射或吸入前列腺素与相当的副作用相关联的或需要显著患者承诺,和内皮素受体拮抗剂波生坦与肝脏毒性的风险增加(发生在患者〜10%)相关联20。西地那非结合口服治疗重症PAH的优势有关于这些患者的肝功能受损肝脏的副作用极好的风险配置文件。
In the current study, two patients died, 1 and 2 months after initiation of sildenafil treatment, respectively. One patient died owing to liver failure in advanced liver cirrhosis due to HHT. This patient was not eligible for liver transplantation due to severe pulmonary hypertension2,4。第二个病人肝硬化由于病毒性肝炎遭遇。尽管联合治疗吸入性伊洛前列素和西地那非,她出现进行性肺血管病变和右心脏衰竭死亡。
虽然名患者已经接受吸入前列腺素与有效剂量,需要进行功能稳定的另外的肺血管活性治疗。Combination of sildenafil add-on therapy with inhaled prostanoids resulted in a favourable improvement after 3 and 12 months, similar to that shown by patients being treated with sildenafil monotherapy. The effects seen in the current study were comparable to those seen in patients with other forms of PAH21,22。在对治疗的反应对于肝脏疾病的起源的差异发现无论是在目前的研究中,也没有在以前的报告1-4。In the current study, patients with a milder degree of liver cirrhosis showed a significant improvement in exercise capacity after 3 months’ sildenafil therapy compared with patients in advanced stages of liver disease (fig. 2⇓)。虽然这种效应可能与样本量小,应该在即将到来的调查,加以考虑。
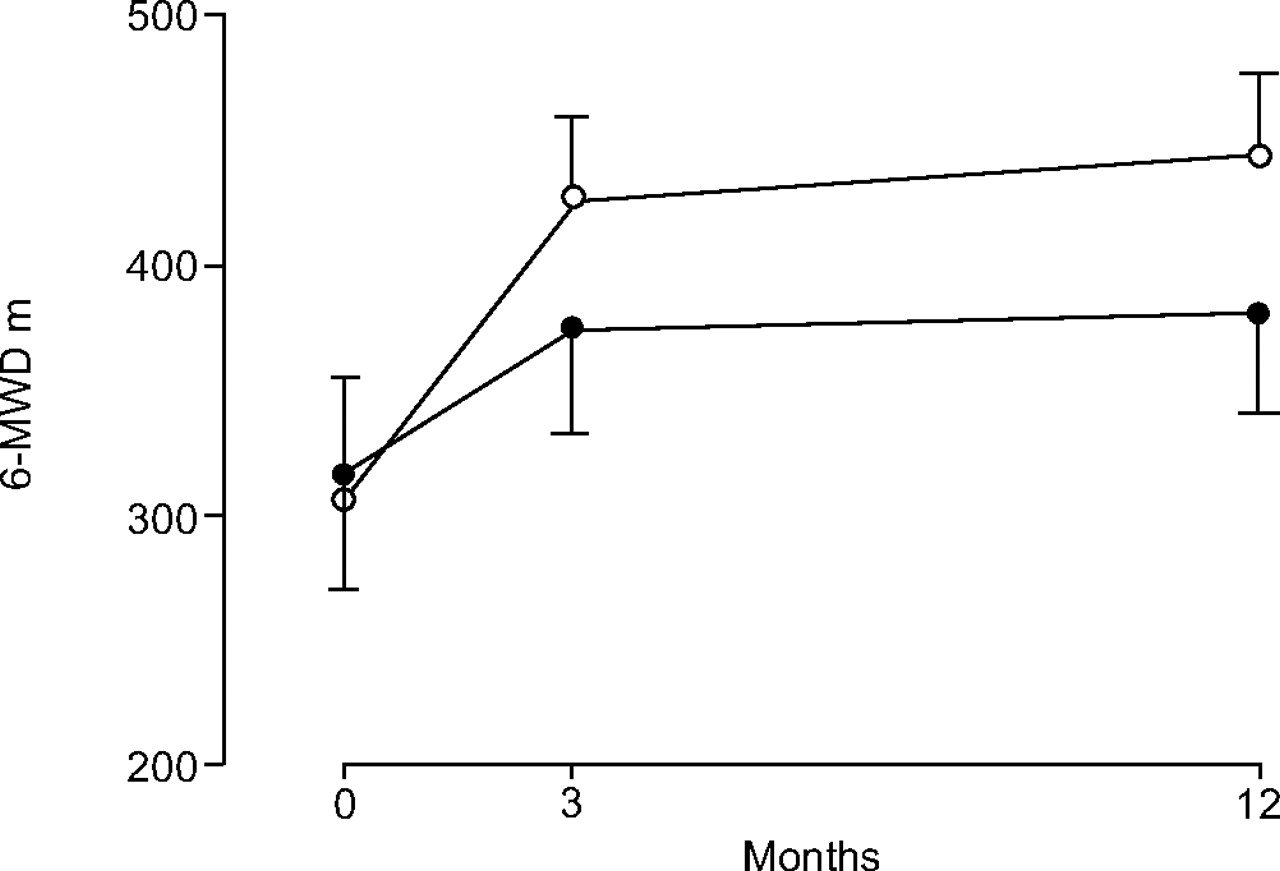
A 6-min walking distance (6-MWD) after 3 and 12 months’ follow-up treatment, comparing sildenafil monotherapy (•; n = 7) and sildenafil and inhaled prostanoids combination therapy (○; n = 5). Data are presented as mean±SEM。有治疗组间差异无统计学显著差异。
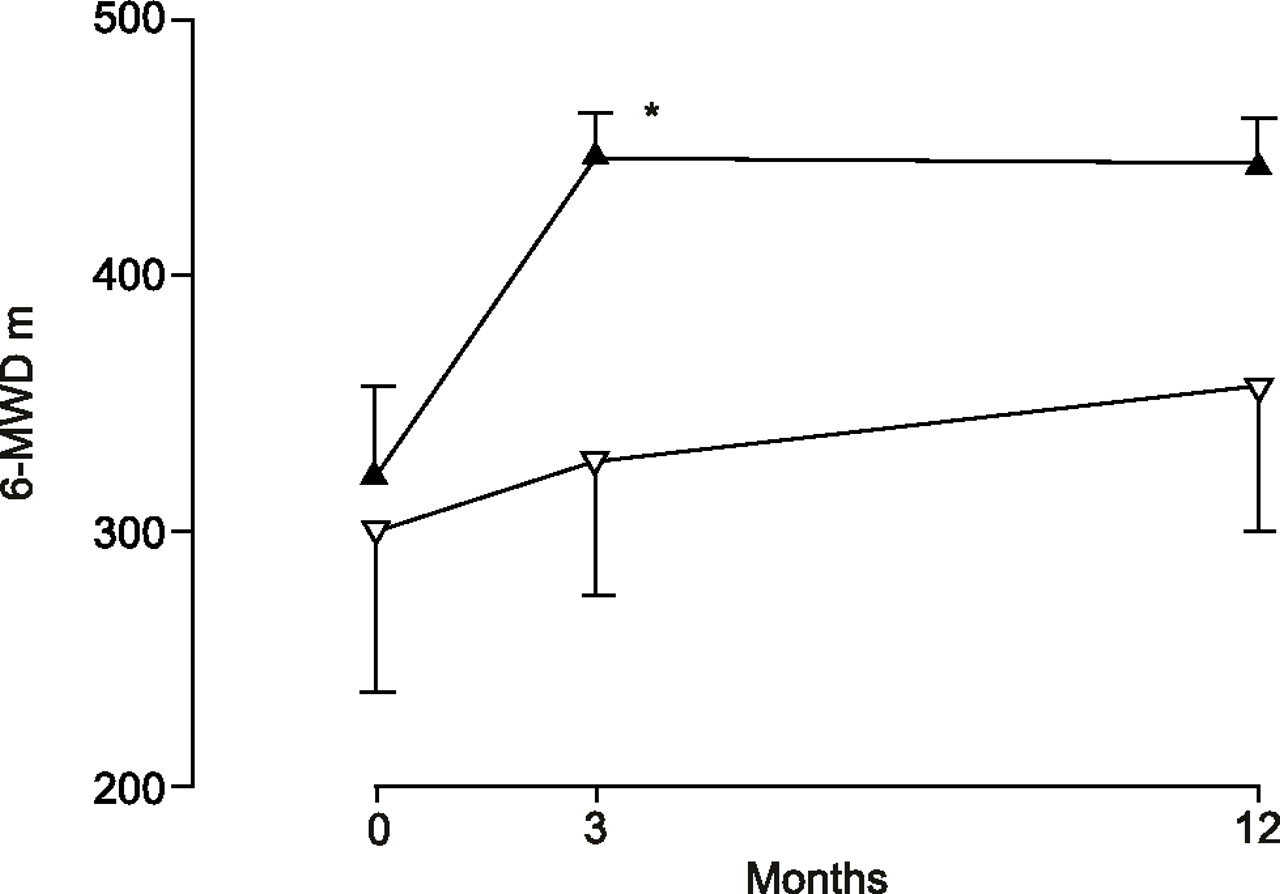
Follow-up after 3 and 12 months’ sildenafil treatment, comparing degrees of hepatic impairment. Data are presented as mean±SEM。Child A: ▴, n = 7; Child B: ▿, n = 5. There was a statistically significant difference between the two groups at 3 months (事后ANOVA)。*:P <0.01与基线。
Although there was a slight deterioration in haemodynamic parameters after 12 months, patients remained in a stable clinical and functional condition. In addition, pro-BNP levels remained stable. In the current study, a sildenafil dose 2.5 times as high as the currently approved dosage for treatment of PAH was used. Sildenafil dosage was not increased further owing to the potential for bleeding.
没有病人在目前的研究经历,同时对慢性西地那非治疗出血事件或需要输血。值得注意的是,有消化道出血的没有报告的事件,如先前报道23,24。两名死者的患者均未见致命性出血事件的迹象,并分别从肝功能衰竭和心脏衰竭,死亡。
目标导向治疗是PAH当前的挑战,具体目标可能是与越来越多的证据,和可用性,联合治疗可达到25。
在目前的研究的患者样品,开始与对慢性吸入前列腺素治疗引线的顶端口服西地那非组合疗法为显著和持续而不显著副作用的血液动力学和功能的改善。然而,进一步的另外的疗法包括静脉注射依前列醇可能会在需要时肝移植计划或患者不联合治疗稳定1。
有在目前的研究主要局限。的肝病患者威力的异构病因相当低的数目表明选择偏倚。亚组分析或潜在的副作用,需要进一步调查。
虽然目前的研究还不足以推断一般治疗建议,受试者所参考的评估和治疗肺动脉高压的大型专业化中心,为肺血管疾病的患者招募。在目前的作者认为,西地那非治疗的反应已经足够明显,同质产生显著的效果。
In conclusion, sildenafil is a safe and well-tolerated therapy in portopulmonary hypertension which may lead to significant clinical, functional and haemodynamic improvement after 3 months and to a sustained response over 12 months either as monotherapy or in combination with inhaled prostanoids.
致谢
目前的研究是E. Steveling的博士论文的一部分。
- 收到2006年2月28日。
- 公认2006年6月15日。
- ©ERS期刊有限公司







{kind=link}
{kind=link}
{kind=link}
{kind=link}