





我们要感谢S.特纳,他在我们工作的关注,我们很高兴的评论提出的方法问题。
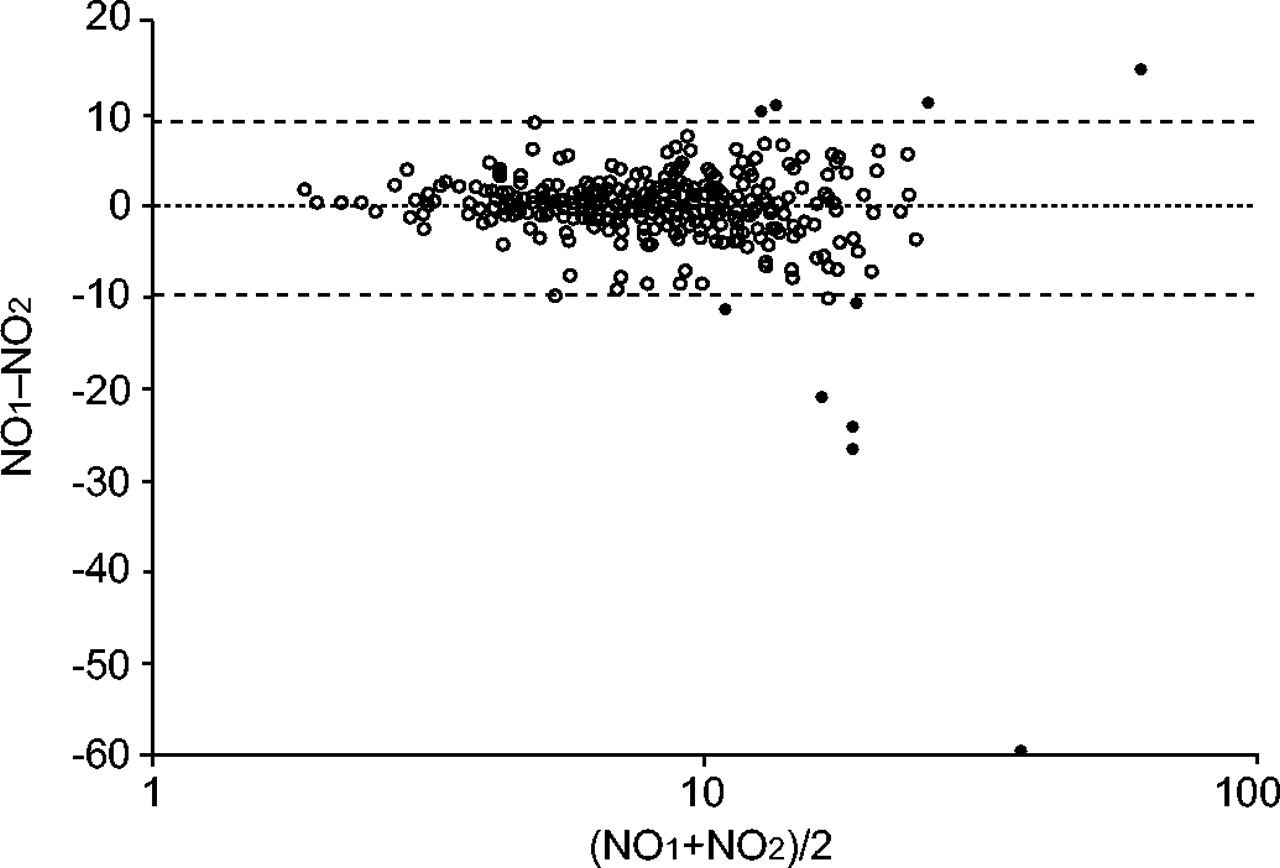
与呼出气一氧化氮的部分的重复性的第一个问题涉及(FeNO的孩子内)测量。在我们的研究中1中,我们观察到在第一和第二之间的良好相关性FeNO的measurements from the children (Spearman r = 0.73; p<0.001). Also, in the majority of the children, the mean difference between the duplicateFeNO的measurements was <5 ppb (89%), whereas, in a small minority of children, the difference was >10 ppb (2%; fig. 1⇓)。为了找到一方面是测量的重复性,而在另一方面孩子们的足够数量的维护之间取得合理的平衡,我们选择了包括所有的孩子对他们来说,重复的区别FeNO的measurements was within 10 ppb. Separate analyses of children for whom the duplicate measurements were within 5 ppb produced similar results. For example, in the total study population, the geometric meanFeNO的values in ppb (95% confidence interval) for children with and without a doctor's diagnosis of asthma were 9.4 (7.6–11.7) and 7.6 (7.3–8.0), respectively (p = 0.06), instead of 10.0 (8.3–12.1) and 7.9 (7.5–8.2), respectively (p<0.05), when duplicate samples were within 10 ppb from each other. With respect to atopy, these numbers were 9.1 (8.0–10.4) and 7.4 (7.0–7.9), respectively (p<0.05), for samples within 5 ppb, and 9.4 (8.4–10.5) and 7.7 (7.2–8.1), respectively (p<0.05), for samples within 10 ppb. So, when more stringent criteria were applied, theFeNO的值不有和没有哮喘或过敏体质的儿童之间更有辨别力。
呼出气一氧化氮的重复部分之间的协议布兰德Altman图(FeNO的)测量,表示重复之间的平均差FeNO的测量(═)和平均差±2SD( - - )。开放和实心圆圈表示的孩子谁之间的区别重复FeNO的measurements was <10 ppb or >10 ppb, respectively. The x-axis is logarithmic.
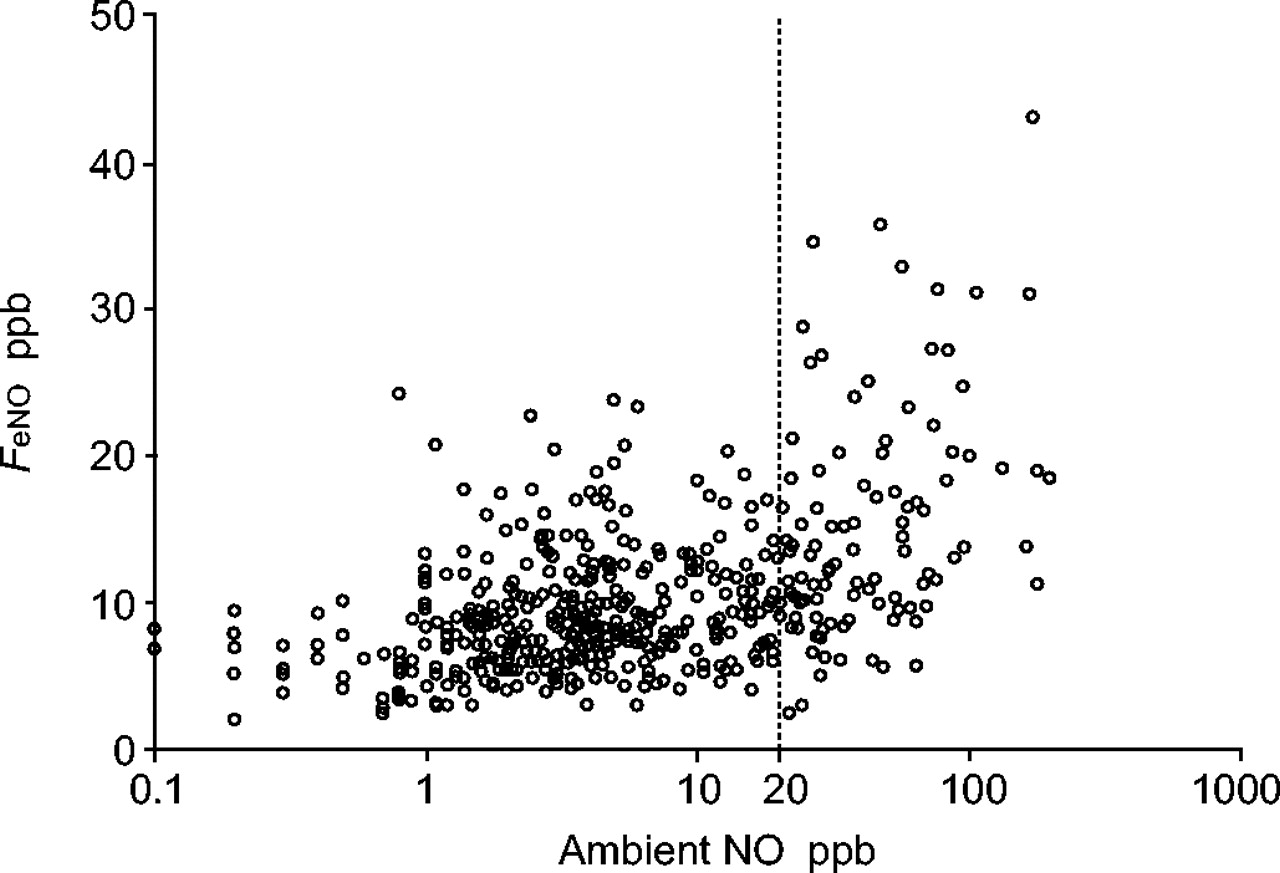
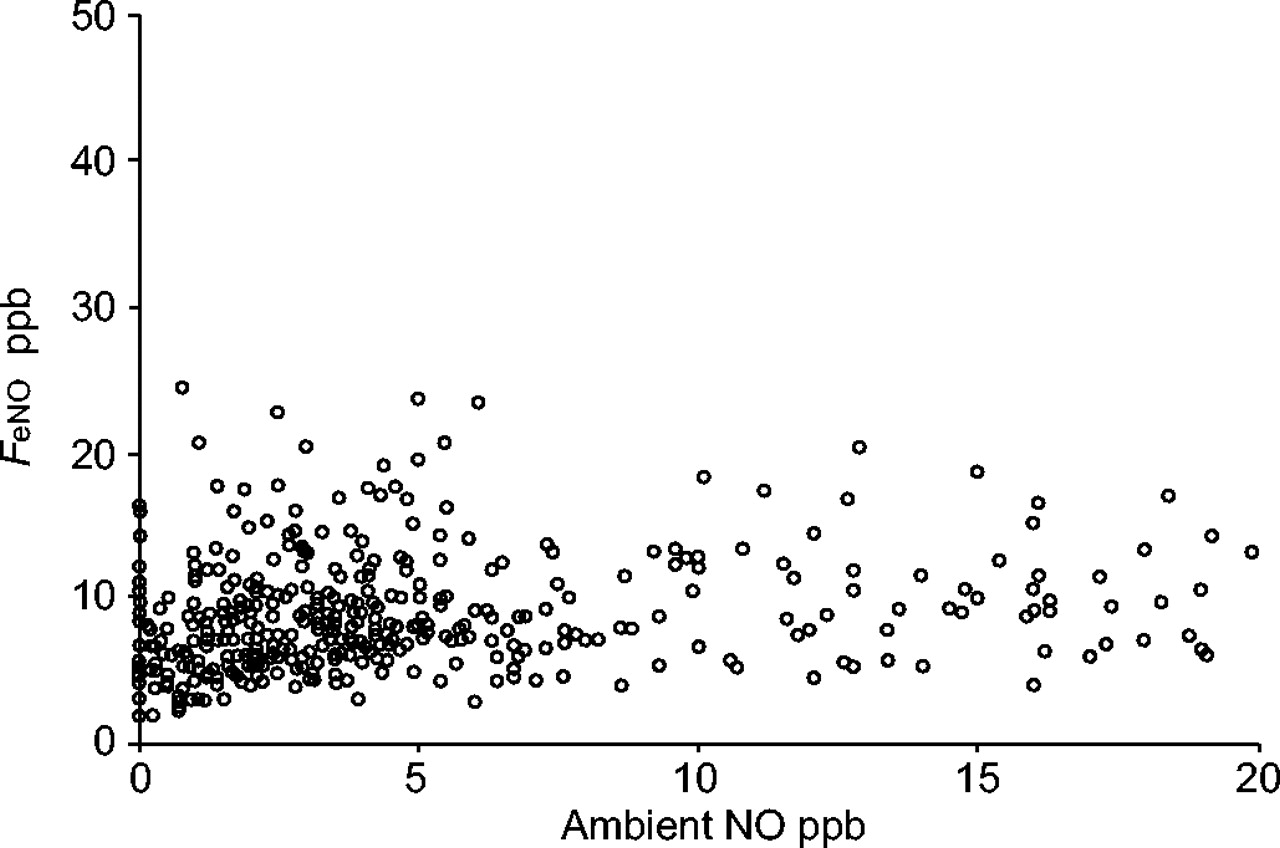
关于环境的一氧化氮的价值观,我们已经检查了它们对呼出气一氧化氮的作用。Since there was no significant influence of ambient nitric oxide levels <20 ppb on the fraction of exhaled nitric oxide values in our study population (figs 2⇓和3⇓), we decided to include all children with ambient nitric oxide levels <20 ppb in the analyses. When the analyses were repeated, including only those children for whom the ambient nitric oxide values were <10 ppb, similar results were observed.
环境的一氧化氮(NO)水平对呼出一氧化氮的分数的影响(FeNO的)值在研究人群。x轴是对数的。
The influence of ambient nitric oxide (NO) levels <20 ppb on the fraction of exhaled nitric oxide (FeNO的)水平在研究人群。
- ©ERS期刊有限公司







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}