





Abstract
Prediction bias in spirometry reference equations can arise from combining equations for different age groups, rounding age or height to integers or using self-reported height.
To assess the bias arising from these sources, the fit of 13 prediction equations was tested against the Global Lungs Initiative (GLI) dataset using spirometric data from 55,136 healthy Caucasians (54% female). The effects on predicted values of using whole-year ageversus定量小数年龄和高度1%的偏差。
In children, the prediction bias relative to GLI ranged from -22% to +17%. Switching equations at 18 yrs of age led to biases of between -846 (-14%) and +1,309 (+38%) mL. Using age in whole years rather than decimal age introduced biases from -8% to +7%, whereas a 1% overestimation of height introduced bias that ranged from +1% to +40%. Bias was greatest in children and adolescents, and in short elderly subjects.
Using a single spirometry equation applicable across all ages and populations reduces prediction bias. Measuring and recording age and height accurately are also essential if bias is to be minimised.
身高和年龄是肺活量参考方程中最重要的解释变量。测量肺活量指标的指南,旨在最大化准确性和精确度,专注于设备,测量程序和质量控制[1]。They do not, however, address the equally important issues of accurate height and age measurement. For example, in the Global Lungs Initiative (GLI) dataset [2],只有45%的高度记录到1毫米的精度,12%的高度是自我报告的,并且在整个年份中记录了45%的年龄,其中许多人被软件舍入围。所有这些都有可能偏向肺活量指标的预测,尤其是在儿童中。
Both height and age appear consistently in adult prediction equations, but in children height is commonly used without age. Examples are P奥尔加等. [3]和wang等. [4](由美国胸腔学会和欧洲呼吸学会(ERS)推荐[188bet官网地址1]在美国),rosenthal等.[5] in the UK (recommended by the British Thoracic Society and the Association of Respiratory Technicians and Physiologists [6]) and Zapletal等. [7] 在欧洲。然而,已经表明,在青春期,年龄,身高和肺活量测定法之间的关系[8,9], and that this can only be accounted for by including age in the equation [9,10]。Thus the omission of age from the equation will generate bias at certain ages in childhood.
In the past, most prediction equations were developed separately for children and adults, with a disjunction in the prediction at the child–adult age boundary (usually around 18–19 yrs). Recently, spirometry reference equations have become available for Caucasians [10] and other ethnic groups [2] from childhood to old age, complete with accurate lower limits of normal. These all-age equations avoid the child–adult disjunction, and they inevitably highlight bias due the disjunction in other equations.
This study aims to address four questions, focusing on forced expiratory volume in 1 s (FEV1) and forced vital capacity (FVC) in Caucasians relative to the GLI [2], namely: how large is the prediction bias 1) for other commonly used spirometry prediction equations, 2) for paediatric prediction equations that omit age, 3) at the child–adult age boundary and 4) due to biases in age and height measurement?
We used data on 54,866 healthy Caucasian lifelong nonsmokers from the GLI [2];24,768 males and 30,098 females aged 6–95 yrs. The paediatric subset comprised of 14,486 boys (height 96.0–198.5 cm) and 14,053 girls (height 100.0–188.0 cm) aged 6–18.99 yrs.
GLI数据集的完整帐户目前正在印刷中[2]。
METHODS
FEV1回答和FVC测量GLI 2012数据集e expressed as per cent of predicted, based on each of the following prediction equations. Children and adolescents: GLI 2012 [2],p奥尔加等. [3], Wang等. [4], Rosenthal等. [5], Zapletal等. [7], QUanjer等. [9], STanojevic等. [10], H安金森等. [11]和k努德森等. [12];成人:GLI 2012 [2], STanojevic等. [10], Crapo等. [13],钢铁和煤炭的欧洲社会[14], Falaschetti等. [15] and the SAPALDIA study [16,17]。
Within the dataset, height was recorded to 1 mm accuracy in 57.2% of those <19 yrs and 33.8% of those ≥19 yrs (n=28,539 and 26,327, respectively). Similarly, age was reported to one decimal place accuracy in 89.2% of subjects <19 yrs and in 16.0% of those ≥19 yrs.
通过将基于小数年龄的预测值与基于截短年龄的年龄进行比较,可以探索整个年龄的记录年龄的影响。还使用高度 +1%偏置计算预测值,以模拟小的测量误差或乐观的自我报告。年龄引入的偏差为0.0-0.99岁(平均值±SD0.30±0.32 in males and 0.26±0.32 yrs in females), while for height the bias was 0.9–2.0 cm (mean±SD1.5±0.24 cm) in males, and 0.8–1.9 cm (mean±SD1.5±0.18 cm) in females. All calculations were performed within the age range specified in published prediction equations, precluding extrapolation beyond valid age ranges.
“ 18岁生日的效果”是从儿科方程的过渡大小,该方程可在≥18岁的受试者中施加至18岁的成人方程。根据各种儿童和成人的预测方程,数据集中发现了386名男孩和404名女孩,并计算出17.99和18.0岁的预测值,从而估计了这一点。2–5,7,9–17]。两个年龄段使用相同的高度。
RESULTS
切换到儿童GLI 2012方程的影响
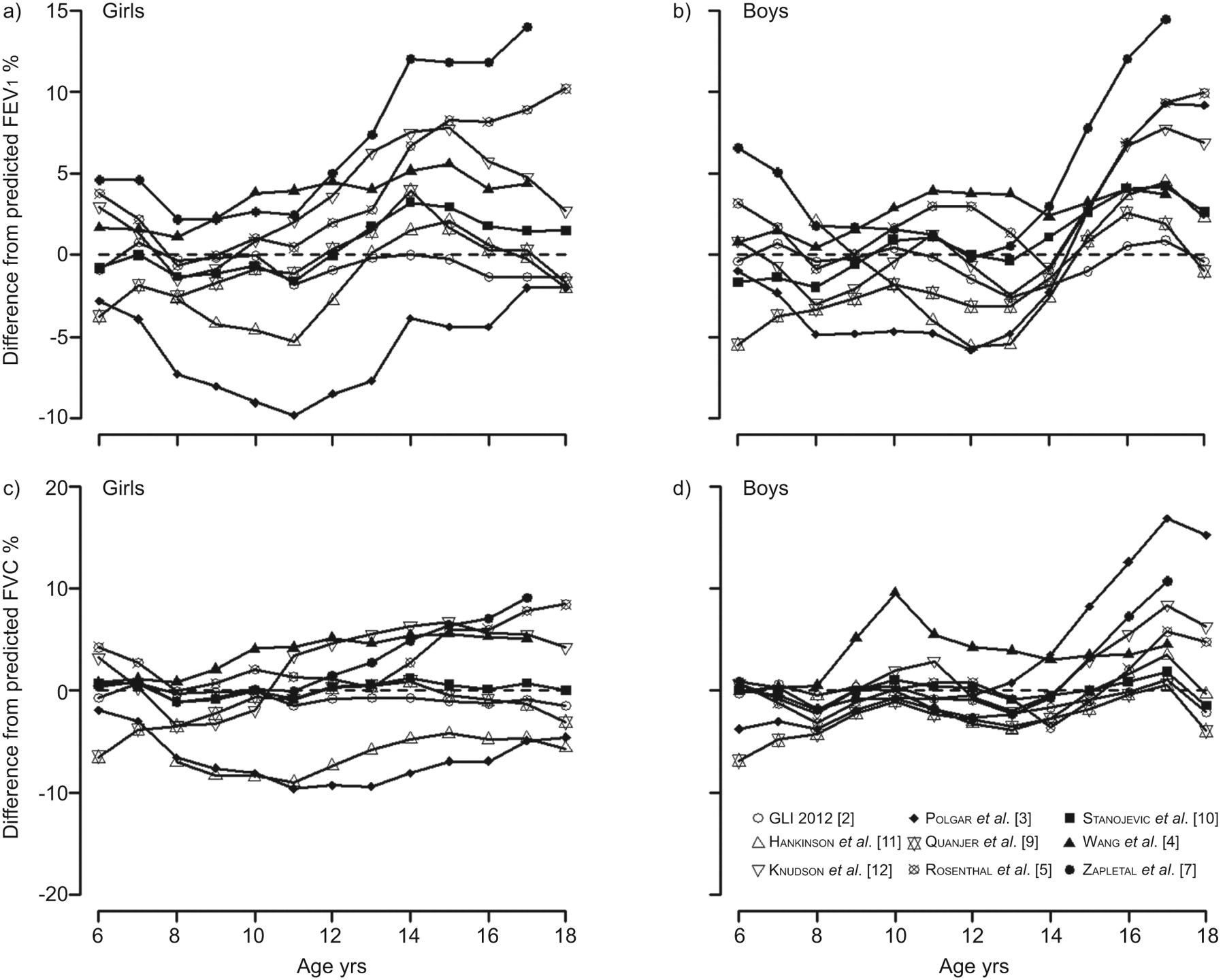
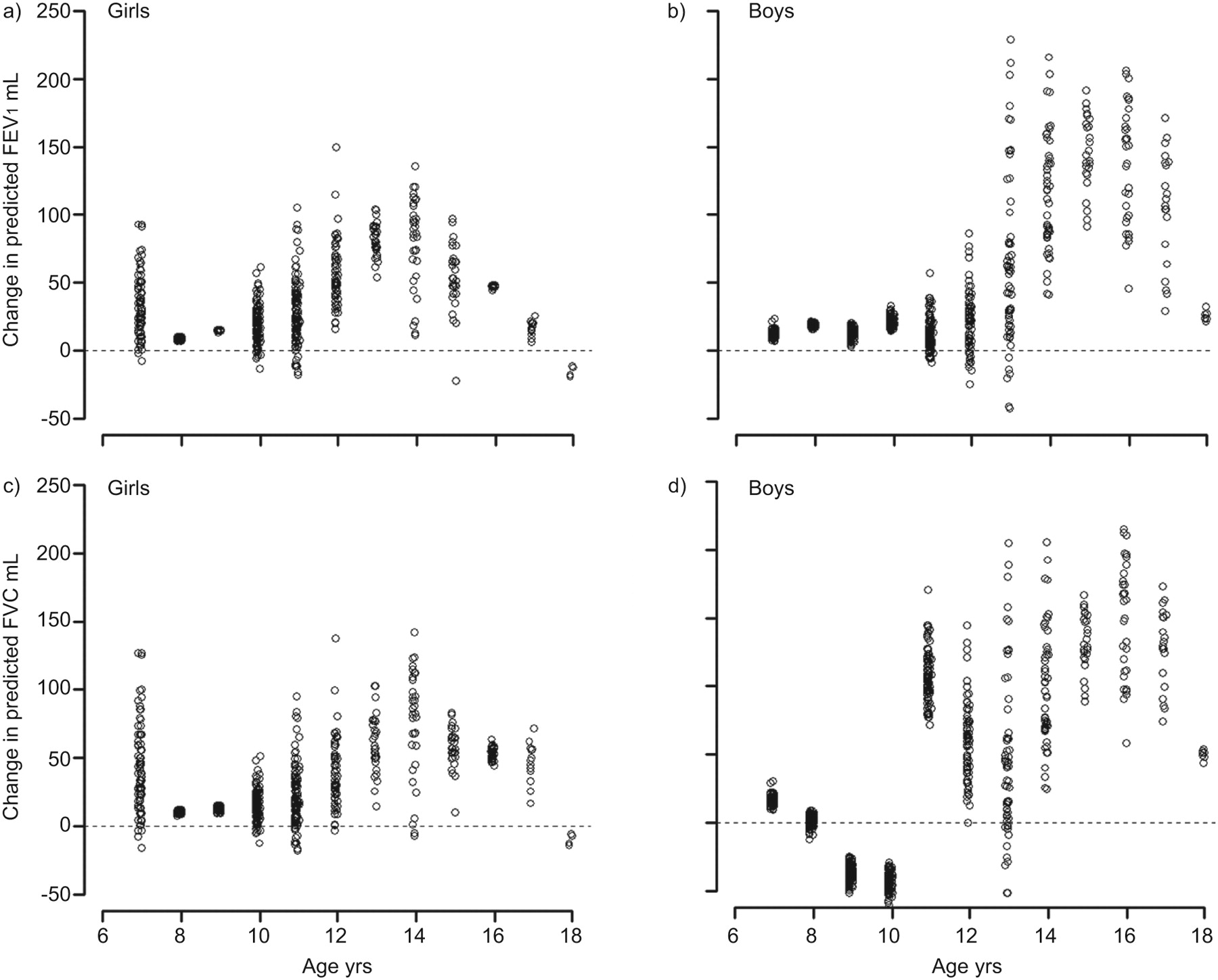
计算每个回归方程的100%预测值的测量值的平均偏差。可以预见的是,GLI 2012的方程[2]和sTanojevic等. [10[]最适合他们共享方法,并且有许多共同的数据,但在增长过程中仍然有略有偏见(如图。1)。The reference equations omitting age as an explanatory variable (P奥尔加等. [3], Rosenthal等. [5]和zapletal等. [7])表现特别差(table 1;如图。1)。
平均与预测值的平均偏差为预测的百分比,对于1 s的强制呼气量(FEV)1) (upper panels) and forced vital capacity (FVC) (lower panels) in girls (left panels) and boys (right panels), when applying prediction equations from various authors to the Global Lungs Initiative (GLI) data. A difference of 0% indicates that the predicted values perfectly match the GLI 2012 data.
孩子的生日效果
从W中的预测值ang等. [4] are based on power functions of height which differ for each full year from 6–18 yrs. We identified 1,987 subjects from the GLI dataset (1,019 boys and 968 girls) who were within 1 month of their birthday, and calculated their Wang predicted values for the ages before and after their birthday (如图。2)。The same height was used for both predictions, as height increment over a month is small. In girls and boys the birthday discontinuities varied from -42 to +229 mL in FEV1, and -65 to +215 mL in FVC.
Differences between predicted values for forced expiratory volume in 1 s (FEV1) and forced vital capacity (FVC) by sex just before and after a birthday (i.e.for the same height), based on the age-specific prediction equations of Wang等. [4]。
When switching to other equations at age 18 yrs (18th birthday effect), the FEV1change in boys ranged between -846 mL (-14%) and +1,309 mL (+38%) (表2)。Findings for FVC and for girls were similar (not shown).
偏见的年龄和身高测量
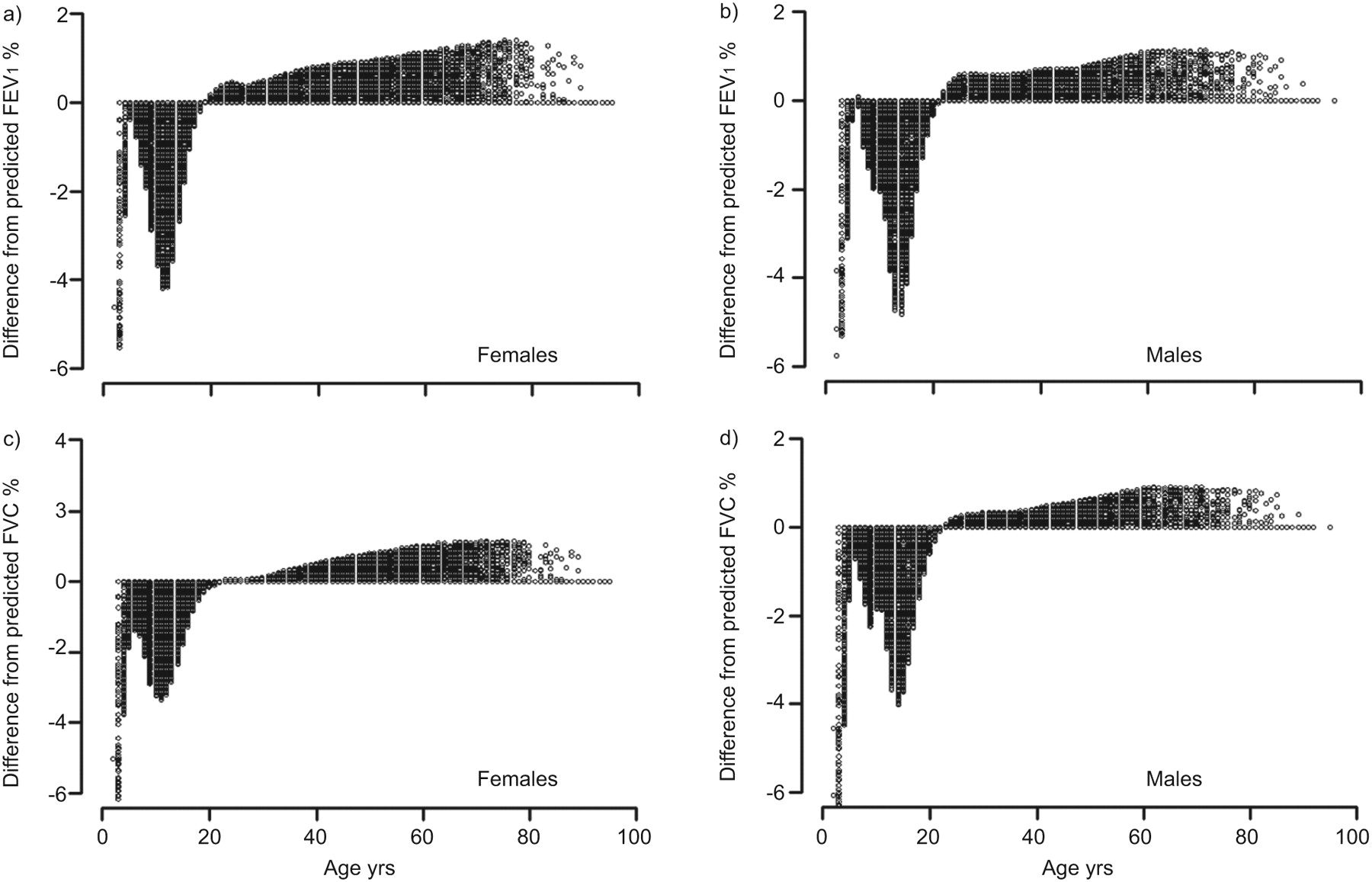
Based on the GLI 2012 equations [2], the percentage bias in FEV1在学龄前儿童和青少年中,由于截断年龄到整个年龄而产生的FVC最大,高达8.5%(如图。3;表3)。With the GLI 2012 [2]和sTanojevicequations [10]高度的1%偏差导致FEV偏见1and FVC of 2.1–2.4% (表3)。截断年龄和夸张的身高减少了童年的偏见(如图。3),但在成年后增加了它。在整个年龄范围内,其他方程式的使用导致-9至 +40%的偏见(表3)。
{kind=link}
{kind=link}
![Differences between predicted values for forced expiratory volume in 1 s (FEV1) and forced vital capacity (FVC) by sex just before and after a birthday (i.e. for the same height), based on the age-specific prediction equations of Wang et al. [4].](http://www.qdcxjkg.com/content/erj/40/1/190/F2.large.jpg?width=800&height=600&carousel=1){kind=link}
{kind=link}
![Percentage bias in predicted forced expiratory volume in 1 s (FEV1) and forced vital capacity (FVC) by sex due to truncating age to whole years. Predicted values according to Global Lungs Initiative, 2012 [2].](http://www.qdcxjkg.com/content/erj/40/1/190/F3.large.jpg?width=800&height=600&carousel=1){kind=link}
{kind=link}
1 s的预测强迫呼气量的偏差百分比(FEV1) and forced vital capacity (FVC) by sex due to truncating age to whole years. Predicted values according to Global Lungs Initiative, 2012 [2]。
DISCUSSION
有几个实际问题,房颤fect the interpretation of lung function values. The current practice to combine reference equations from different populations and different age ranges introduces biases ranging from -14% to 38% at the transition from adolescence to adulthood. This range can be converted to the z-score scale by dividing by the coefficient of variation, which at this age is ∼12% [2]。因此,偏置范围为-1.2和+3.2 z得分单元,对临床围绕正常下限的测试结果的临床解释带来了严重的后果。截断年龄或使用自我报告的高度会导致进一步的偏见。通过应用跨越所有年龄段的全局参考方程,并使用身高和年龄准确的度量准确至少一个小数位,可以极大地改善肺活量测量结果的解释。
With two exceptions which shared many of the data and used the same statistical approach [2,10],预测方程对GLI数据集的拟合很差,方程之间存在很大的差异。这导致了许多清醒的结论。关于预测方程的当前情况是高度令人满意的,尤其是在小儿年龄范围内。有很多肺活量测定方程;一个非竭尽的摘要列出了120个此类等式[18]。However, the piecemeal approach of dividing the human lifespan into small sections inevitably leads to disjunctions at the age group boundaries (表2)。These arise mainly from the use of different models, which may fit the data poorly, and from the use of population samples that are often small and only poorly representative of the population [2,19]。Thus there is an urgent need for a consistent evidence-based approach towards the construction and use of reference values. Until recently no statistical techniques allowed accurate and continuous description of pulmonary function from childhood to old age. However, with the advent of new techniques, notably the GAMLSS technique [10,20–23] it is now possible to summarise pulmonary function across the whole age range. In addition, it allows the lower limit of normal (usually the fifth percentile), which varies appreciably with age [10,15,16,22], to be modelled properly. It is costly and time-consuming to collect sufficient data covering the entire age range. However, collating good quality data from different studies has been shown to be a valid alternative [9,10,22,24]。
With the advent of automated pulmonary function machines, laboratories have to decide which prediction equations to use from the selection provided by the manufacturer. Few laboratories are sufficiently informed about the alternatives, and in practice many use the manufacturer's default choice. Such defaults often include equations that include a transition from adolescence to adulthood. Even in institutions with respiratory disease training programmes, people are often unaware of the reference values used in their institute [25,26]。参考标准的变化,尤其是在未经通知的情况下,可能会对诊断,转诊,治疗,术前评估,残疾评级甚至肺移植引用以及串行测量的解释[27–29]。迫切需要使用跨越童年到老年的预测方程[2,10];the GLI 2012 equations achieve this [2],并提供对四个族裔有效的额外优势,从而消除了对任意种族矫正因素的需求。
The second major finding is that biased age and height measurements can lead to considerable bias in predicted values, which naturally propagate into the lower limits of normal. For example, using the GLI 2012 reference [2], a 1-yr age bias due to truncating age to the last birthday, can lead to a bias in predicted values of up to 8.5% (表3)。This may be due simply to the common practice of entering age in whole years, or the failure of software to compute decimal age as the difference between test date and birth date. Truncating age biases the predicted value downwards in children, particularly in puberty, and upwards in adults (如图。3)。高度的偏置仅偏差 +1%会导致预测FEV的增加1and FVC by between 0.9% and 40%. In reality, biases greater than this can easily occur purely due to a poorly calibrated stadiometer, or using self-reported height. Importantly the two biases are cumulative, leading to significant errors in predicted spirometric outcomes.
高度高达6.9厘米的错误可能是由于使用自我报告的高度[30], as has been reported for several different ethnic groups [30–34]。Males tend to overestimate their height more than females [35]。Over-reporting height also increases with age; thus on average males and females aged 65–79 yrs over-reported by 2.3 and 1.6 cm, respectively, and those aged 80 yrs or older by 2.6 and 3.3 cm [35]。另外,如果使用先前记录的值,则可能发生高度错误:在快速增长期间的儿童中,在发生身高损失的老年人中。请注意,尽管该研究仅限于高加索人,但这些发现也适用于其他种族(结果未显示)。
为了准确解释肺功能,必须准确地将年龄和身高准确地输入年龄和身高。这可以通过使用需要输入出生日期以及测量日期的软件来实现。高度应用校准的标准计测量,受试者直立站立,没有鞋子,肩膀,臀部和高跟鞋在墙壁或标准计上平坦,头部倾斜,使下轨道水平和外听肉类(法兰克福平面)是等级;测量应记录到最近的0.1厘米。理想情况下,应使用两个测量的平均值。不应使用英寸,因为转换为厘米可能会产生错误。在推导新的预测方程式时,还需要准确记录的高度和年龄(达到小数点的精度)。
结论
There are large differences in frequently used predicted values according to different authors. Consequently, a transition from one to another set of reference equations can have profound clinical consequences. Therefore, final reports should always name the set of reference values used, so that this can be taken into account when interpreting test results. Also in any institute the transition to new reference equations should always be properly announced, and the consequences clearly explained to medical practitioners. The use of modern prediction equations valid from childhood to old age, derived from large datasets [2,10] and applicable to different ethnic groups [2], obviates the need to change from one set of equations to another, and so avoids age-related disjunctions. It also provides a worldwide standard for the interpretation of spirometric test results.
Acknowledgments
Members of the ERS Global Lungs Initiative (www.lungfunction.org) are as follows. Chairs: J. Stocks, X. Baur, G.L. Hall and B. Culver; analytical team: P.H. Quanjer, S. Stanojevic, T.J. Cole and J. Stocks; additional members of the steering committee: J.L. Hankinson, P.L. Enright, J.P. Zheng and M.S.M. Ip. Persons and centres contributing data on Caucasians to the Global Lung Initiative are as follows. H.G.M. Arets, Dept of Pediatric Pulmonology, Wilhelmina Children's Hospital, University Medical Center Utrecht, Utrecht, the Netherlands; C. Bárbara, The Portuguese Society of Pneumology, Lisbon, Portugal; C.S. Beardsmore, Dept of Infection, Immunity and Inflammation (Child Health), University of Leicester, Leicester, UK; H. Ben Saad, Laboratory of Physiology, Faculty of Medicine, Sousse, University of Sousse, Tunisia; B. Brunekreef, Institute for Risk Assessment Sciences, Universiteit Utrecht, Utrecht, the Netherlands; P.G.J. Burney, National Heart and Lung Institute, Imperial College, London, UK; D. Dockery, Dept of Environmental Health, Dept of Epidemiology, Boston, MA, USA; H. Eigen, Section of Pulmonology and Intensive Care, James Whitcomb Riley Hospital for Children, Indiana University School of Medicine, Indianapolis, IN, USA; E. Falaschetti, Health Survey for England 1995–1996 (HSE), International Centre for Circulatory Health, National Heart and Lung Institute, Imperial College, London, UK; B. Fallon, Respiratory Laboratory, Nepean Hospital, Penrith, Australia; M. Gappa, LUNOKID study group, Children's Hospital and Research Institute, Marienhospital Wesel, Wesel, Germany; M.W. Gerbase, Division of Pulmonary Medicine, University Hospitals of Geneva, Geneva, Switzerland, and the SAPALDIA cohort study; T. Gislason, Landspitali University Hospital, Dept of Allergy, Respiratory Medicine and Sleep, Reykjavik, Iceland; C.J. Gore, Physiology Department, Australian Institute of Sport, Belconnen, Australia; A. Gulsvik, Dept of Thoracic Medicine, Institute of Medicine, University of Bergen, Bergen, Norway; G.L. Hall, Respiratory Medicine, Princess Margaret Hospital for Children, Perth, Australia; J.L. Hankinson, NHANES, NHANES III Special data sets, Hankinson Consulting, Valdosta, GA, USA; A.J. Henderson, ALSPAC (www.bris.ac.uk/alspac), University of Bristol, Bristol, UK; C. Janson, Dept of Medical Sciences, Respiratory Medicine and Allergology, Uppsala University, Uppsala, Sweden; C. Jenkins, Woolcock Institute of Medical Research, Sydney, Australia; A. Jithoo, University of Cape Town Lung Institute, Cape Town, South Africa; S. Karrasch, Institute and Outpatient Clinic for Occupational, Social and Environmental Medicine, Hospital of the Ludwig-Maximilians-University, Munich, Germany (KORA study); G.S. Kerby, Lung Function Measures in Preschool Children with Cystic Fibrosis study group, University of Colorado Denver School of Medicine Pulmonary Medicine, The Children's Hospital, Aurora, CO, USA; J. Kühr, Klinik für Kinder- und Jugendmedizin, Städtisches Klinikum Karlsruhe, Karlsruhe, Germany; S. Kuster, Lungenliga Zürich, Zürich, Switzerland (LuftiBus study); A. Langhammer, The HUNT Study, HUNT Research Centre, NTNU, Verdal, Norway; S. Lum, Portex Respiratory Unit, UCL, Institute of Child Health, London, UK; D.M. Mannino, University of Kentucky, Lexington, KY, USA; G. Marks, Woolcock Institute of Medical Research, Sydney, Australia; A. Miller, Beth Israel Medical Center, New York, NY, USA; E. Nizankowska-Mogilnicka, Division of Pulmonary Diseases, Dept of Medicine, Jagiellonian University School of Medicine, Cracow, Poland; W. Nystad, Division of Epidemiology, Norwegian Institute of Public Health, Oslo, Norway; R. Pérez-Padilla, Instituto Nacional de Enfermedades Respiratorias, Mexico DF, Mexico (PLATINO study); P. Piccioni, SC Pneumologia CPA ASL Torino 2, Torino, Italy; F. Pistelli, Pulmonary and Respiratory Pathophysiology Unit, Cardiothoracic Department, University Hospital of Pisa and Pulmonary Environmental Epidemiology Unit, CNR Institute of Clinical Physiology, Pisa, Italy; P.H. Quanjer, Dept of Pulmonary Diseases, and Dept of Pediatrics, Erasmus Medical Centre, Erasmus University, Rotterdam, the Netherlands; M. Rosenthal, Royal Brompton Hospital, London, UK; H. Schulz, Institute of Epidemiology I, Helmholtz Zentrum München, German Research Center for Environmental Health, Neuherberg, Germany (KORA study); S. Stanojevic, Portex Respiratory Unit, UCL Institute of Child Health, London, UK (Asthma UK Growing Lungs Initiative,www.growinglungs.org.uk),儿童健康评估科学和呼吸医学,加拿大多伦多的病童医院;J.B. Soriano,Cimera的流行病学与临床研究计划,Recinte医院Joan March,Illes Balears,西班牙(Framingham研究);厕所。谭,不列颠哥伦比亚大学,不列颠哥伦比亚大学,加拿大温哥华大学心血管和肺部研究中心;W. Tomalak,波兰州拉布卡分公司国家TBC和肺部疾病研究所呼吸系统生理病理学系;S.W.特纳(Turner),西顿研究小组,英国阿伯丁大学阿伯丁大学儿童健康部;D. Vilozni,Edmond和Lili Safra儿童医院的儿科肺部,Sheba医疗中心Ramat-Gan,隶属于以色列Tel-Aviv的Sackler医学院,以色列电视台;H. Vlachos,加拿大QC魁北克省舍布鲁克大学呼吸医学科儿科系;S. West,澳大利亚悉尼Westmead医院呼吸功能实验室; E.F.M. Wouters, Maastricht University Medical Center, Maastricht, the Netherlands; D. Zagami, Lung Function Laboratory, Gold Coast Hospital, Southport, Australia.
Footnotes
Statement of Interest
没有人宣布。
- 已收到2011年9月16日。
- Accepted2011年12月4日。
- ©ERS 2012
REFERENCES










