Abstract
BackgroundThe coronavirus disease 2019 (COVID-19) outbreak is evolving rapidly worldwide.
ObjectiveTo evaluate the risk of serious adverse outcomes in patients with COVID-19 by stratifying the comorbidity status.
Methods我们分析数据从1590例实验室确认的spitalised patients from 575 hospitals in 31 provinces/autonomous regions/provincial municipalities across mainland China between 11 December 2019 and 31 January 2020. We analysed the composite end-points, which consisted of admission to an intensive care unit, invasive ventilation or death. The risk of reaching the composite end-points was compared according to the presence and number of comorbidities.
Results平均年龄为48.9岁,686名(42.7%)是女性。严重案例占研究人口的16.0%。131(8.2%)患者达到复合终点。报告的399(25.1%)具有至少一种合并症。最普遍的合并症是高血压(16.9%),其次是糖尿病(8.2%)。130名(8.2%)患者报告有两个或多个合并症。调整年龄和吸烟状态后,COPD(HR(95%CI)2.681(1.424-5.048)),糖尿病(1.59(1.03-2.45)),高血压(1.58(1.07-2.32))和恶性肿瘤(3.50(1.60(1.60)7.64))是到达综合终点的危险因素。患有至少一种合并症的患者的危险比(95%CI)为1.79(1.16-2.77),两种或多种合并症的患者中的至少一个合并症。
结论在实验室确诊的Covid-19病例中,任何合并症的患者都会产生较差的临床结果。更多的合并症也与较差的临床结果相关。
Abstract
The presence and number of comorbidities predict clinical outcomes of COVID-19http://bit.ly/3b9w5.
介绍
Since November 2019, the rapid outbreak of coronavirus disease 2019 (COVID-19), which arose from severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection, has recently become a public health emergency of international concern [1]。COVID-19 has contributed to an enormous adverse impact globally. As of 10 March 2020 there have been 113 702 laboratory confirmed cases and 4012 deaths globally [2]。
根据最新报道,Covid-19的临床表现是异质的[3–12]。在入院时,20-51%的患者报告为至少一种合并症,糖尿病(10-20%),高血压(10-15%)和其他心血管和脑血管疾病(7-40%)最常见[3,4,6]。Previous studies have demonstrated that the presence of any comorbidity has been associated with a 3.4-fold increased risk of developing acute respiratory distress syndrome in patients with H7N9 infection [13]。As with influenza [14–18], SARS-CoV [19] and Middle East Respiratory Syndrome coronavirus (MERS-CoV) [20–28], COVID-19 is more readily predisposed to respiratory failure and death in susceptible patients [4,5]。Nonetheless, previous studies have had certain limitations in study design including the relatively small sample sizes and single centre observations. Studies that address these limitations are needed to explore the factors underlying the adverse impact of COVID-19.
我们的目标是根据合并症的数量和类型评估Covid-19患者患者严重不良结果的风险,从而揭示亚群,预后较差。
Methods
数据源和数据提取
This was a retrospective case study that collected data from patients with COVID-19 throughout China, under the coordination of the National Health Commission which mandated the reporting of clinical information from individual designated hospitals that admitted patients with COVID-19. This study is approved by the ethics committee of the First Affiliated Hospital of Guangzhou Medical University. After careful review of medical charts, we compiled the clinical data of laboratory confirmed hospitalised cases from 575 hospitals (representing 31.7% of the certified hospitals admitting patients with COVID-19) between 11 December 2019 and 31 January 2020. The diagnosis of COVID-19 was made based on the World Health Organization interim guidance [29]。因为数据提取的紧迫性,排版lete random sampling could not be applied in our settings. All clinical profiles outside the Hubei province were centrally provided by the National Health Commission. Three respiratory experts from Guangzhou were dispatched to Wuhan for raw data extraction from Wuhan JinYinTan Hospital where most cases in Wuhan were located. Our cohort included 132 patients from Wuhan JinYinTan Hospital, and one each from 338 hospitals. Our cohort represented the overall situation as of 31 January 2020, taking into account the proportion of hospitals (~25%) and patient number (1590 (13.5%) out of 11 791 cases), as well as the broad coverage (covering all major provinces/cities/autonomous regions). Confirmed cases denoted the patients whose high throughput sequencing or real-time, reverse-transcription PCR assay findings for nasal and pharyngeal swab specimens were positive [3]。有关详细信息,请参阅supplementary material。The interval between the potential earliest date of transmission source contacts (wildlife, suspected or confirmed cases) and the potential earliest date of symptom onset (即咳嗽,发烧,疲劳和骨骼)用于计算潜伏期。由于最新日期被记录在一些持续接触污染源的患者中,因此<1天的潜伏期不包括在我们的分析中。孵化期基于划定了划定了特定暴露日期的患者。
The clinical data (including recent exposure history, clinical symptoms and signs, comorbidities, and laboratory findings upon admission) were reviewed and extracted by experienced respiratory clinicians, who subsequently entered the data into a computerised database for further double checking of all cases. Manifestations on chest radiograph or computed tomography (CT) was summarised by integrating the documentation or description in medical charts and, if available, a further review by our medical staff. Major disagreement of the radiologic manifestations between the two reviewers was resolved by consultation with another independent reviewer. Because the disease severity reportedly predicted poorer clinical outcomes of avian influenza [13], patients were classified as having severe or non-severe COVID-19 based on the 2007 American Thoracic Society Infectious Disease Society of America guidelines [30],考虑到其全球接受社区获得的肺炎的严重程度分层,尽管病毒性肺炎患者没有验证没有验证。预测性监护单元(ICU)入学和死亡率的预测能力已验证[31,32]。Briefly, severe cases denoted at least one major criterion (septic shock requiring vasoactive medications, or respiratory failure requiring mechanical ventilation), or at least three minor criteria (respiratory rate ≥30 breaths·min−1, oxygen index ≤250, multiple lobe infiltration, delirium or loss of consciousness, blood urea nitrogen ≥20 mg·dL−1,血白细胞计数≤4000个细胞·DL−1, blood platelet count ≤100 000 cells·dL−1,体温<36°C,和低血压需要维持血压的血管活性药物)。
根据患者的入学的自我报告确定了合并症。初始被治疗为分类变量(是的versus否)并随后根据数字分类(单个versus多)。此外,根据器官系统(即呼吸,心血管,内分泌)。分类为同一器官系统的合并症(即coronary heart disease, hypertension) would be merged into a single category.
我们研究的主要终点是一种复合措施,包括对ICU,侵入性通气或死亡的录取。采用这种复合措施,因为所有个体组分都是H7N9感染的严重结果[13]。次要终点是死亡率。
Statistical analysis
用SPSS软件进行统计分析(版本23.0; SPSS,芝加哥,美国,美国)。没有正式的示例大小估算是因为在Covid-19上没有任何公开的全国范围的数据。尽管如此,我们的样本大小被认为足以为国家患者人口的代表性提供统计分析。连续变量呈现为平均值±sdor median (interquartile ranges (IQR)) as appropriate, and the categorical variables were presented as counts and percentages. Since no random sampling was conducted, all statistical analyses were descriptive and no p-values were presented for the statistical comparisons except for the Cox proportional hazards regression model. Cox proportional hazards regression models were applied to determine the potential risk factors associated with the composite end-points, with the hazard ratio and 95% confidence interval being reported. Our findings indicated that the statistical assumption of proportional hazards analysis was not violated. Moreover, a Cox regression model was considered more appropriate than a logistic regression model because it took into account the potential impact of the various durations of follow-up from individual patients. Age and smoking status were adjusted for in the proportional hazards regression model because they had been recognised as the risk factors of comorbidities even in the general population. Smoking status was stratified as current smoker, ex-smoker and never-smoker in the regression models.
Results
Demographic and clinical characteristics
The National Health Commission diagnosed 11 791 patients in China with laboratory confirmed COVID-19 as of 31 January 2020. At this time-point, for data cut-off, our database included 1590 cases from 575 hospitals in 31 province/autonomous regions/provincial municipalities (refer tosupplementary material)。Of these 1590 cases, mean age was 48.9 years. 686 (42.7%) patients were female. 647 (40.7%) patients were managed inside the Hubei province, and 1334 (83.9%) patients had contact history with Wuhan city. The most common symptom was fever on or after hospitalisation (88.0%), followed by dry cough (70.2%). Fatigue (42.8%) and productive cough (36.0%) were less common. At least one abnormal chest CT manifestation (including ground-glass opacities, pulmonary infiltrates and interstitial disorders) was identified in >70% of patients. Severe cases accounted for 16.0% of the study population. 131 (8.2%) patients reached the composite end-points during the study (table 1)。总的来说,中位数(IQR)随访时间为10(8-14)天。
Covid-19的合并症和临床特征和结果
Of the 1590 cases, 399 (25.1%) reported having at least one comorbidity. The prevalence of specific comorbidities was: hypertension (n=269, 16.9%), other cardiovascular diseases (n=59, 3.7%) cerebrovascular diseases (n=30, 1.9%), diabetes (n=30, 8.2%), hepatitis B infections (n=28, 1.8%), COPD (n=24, 1.5%), chronic kidney diseases (n=21, 1.3%), malignancy (n=18, 1.1%) and immunodeficiency (n=3, 0.2%). None of the cases had doctor-diagnosed asthma. At least one comorbidity was seen more commonly in severe cases than in non-severe cases (32.8%versus10.3%). Patients with at least one comorbidity were older (mean age 60.8versus44.8岁),更有可能呼吸急促(41.4%versus17.8%),恶心或呕吐(10.4%versus4.3%), and tended to have abnormal chest radiograph manifestations (29.2%versus15.1%) (table 1)。
合并症数量的Covid-19分层的临床特征和结果
我们进一步确定了130名(8.2%)的患者,报告有两个或多个合并症。在严重的病例中比在非严重病例中更常见了两种或更多种可混合性(40.0%versus29.4%). Patients with two or more comorbidities were older (mean age 66.2versus58.2 years), were more likely to have shortness of breath (55.4%versus34.1%),恶心或呕吐(11.8%versus9.7%), unconsciousness (5.1%versus1.3%)并具有较少的异常胸部射线照片(20.8%versus23.4%)与有一个合并症的患者相比(table 2)。
Clinical characteristics and outcomes of COVID-19 stratified by organ systems of comorbidities
A total of 269 (16.9%) patients reported hypertension, 59 (3.7%) reported cardiovascular diseases, 30 (1.9%) reported cerebrovascular diseases, 30 (8.2%) reported diabetes, 28 (1.8%) reported hepatitis B infections, 24 (1.5%) reported COPD, 21 (1.3%) reported chronic kidney diseases, 18 (1.1%) reported malignancy and three (0.2%) reported immunodeficiency. Severe cases were more likely to have hypertension (32.7%versus12.6%),心血管疾病(33.9%versus15.3%)、脑血管疾病(50.0%versus15.3%), diabetes (34.6%versus14.3%),乙型肝炎感染(32.1%versus15.7%), COPD (62.5%versus15.3%),慢性肾疾病(38.1%versus15.7%) and malignancy (50.0%versus15.6%) compared with non-severe cases. Furthermore, comorbidities were more common in patients treated in the Hubei province compared with those managed outside the Hubei province as well as patients with a Wuhan exposure history compared with those without (table 3)。
预后分析
Overall, 131 (8.3%) patients reached the composite end-points during the study. 50 (3.1%) patients died, 99 (6.2%) were admitted to the ICU and 50 (3.1%) received invasive ventilation. The composite end-point was documented in 77 (19.3%) patients who had at least one comorbidity as opposed to 54 (4.5%) patients without comorbidities. 37 (28.5%) patients had two or more comorbidities. Significantly more patients with hypertension (19.7%versus5.9%), cardiovascular diseases (22.0%versus7.7%),脑血管疾病(33.3%versus7.8%), diabetes (23.8%versus6.8%),COPD(50.0%)versus7.6%), chronic kidney diseases (28.6%versus8.0%)和恶性肿瘤(38.9%)versus7.9%)与没有(table 3)。
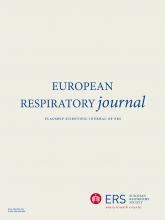
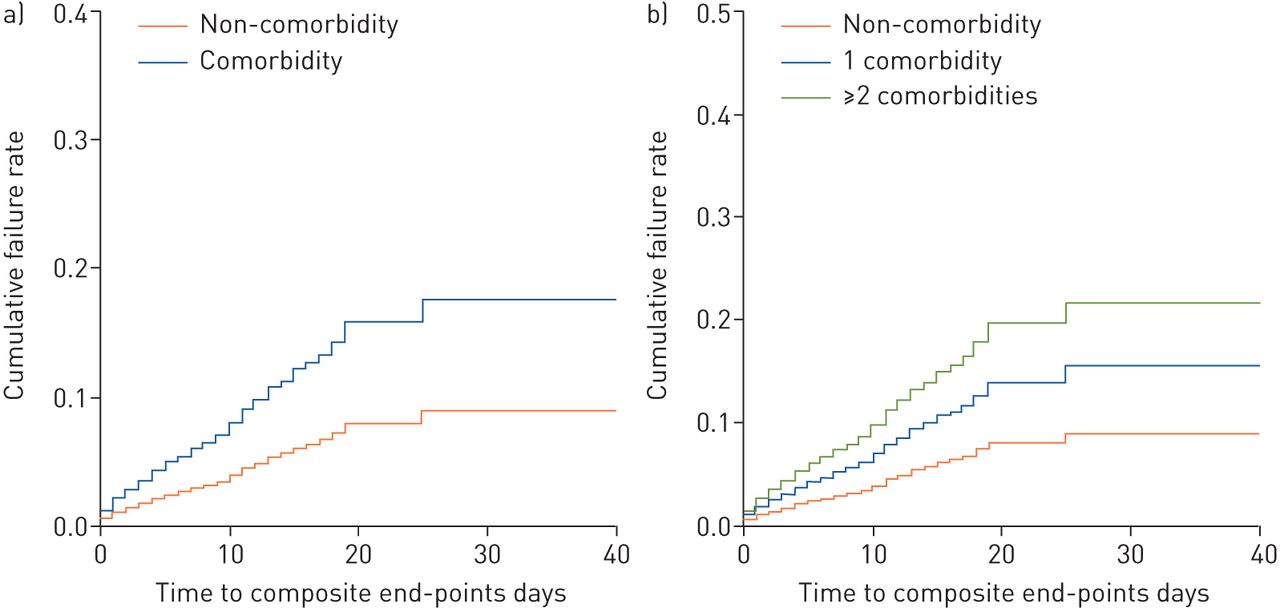
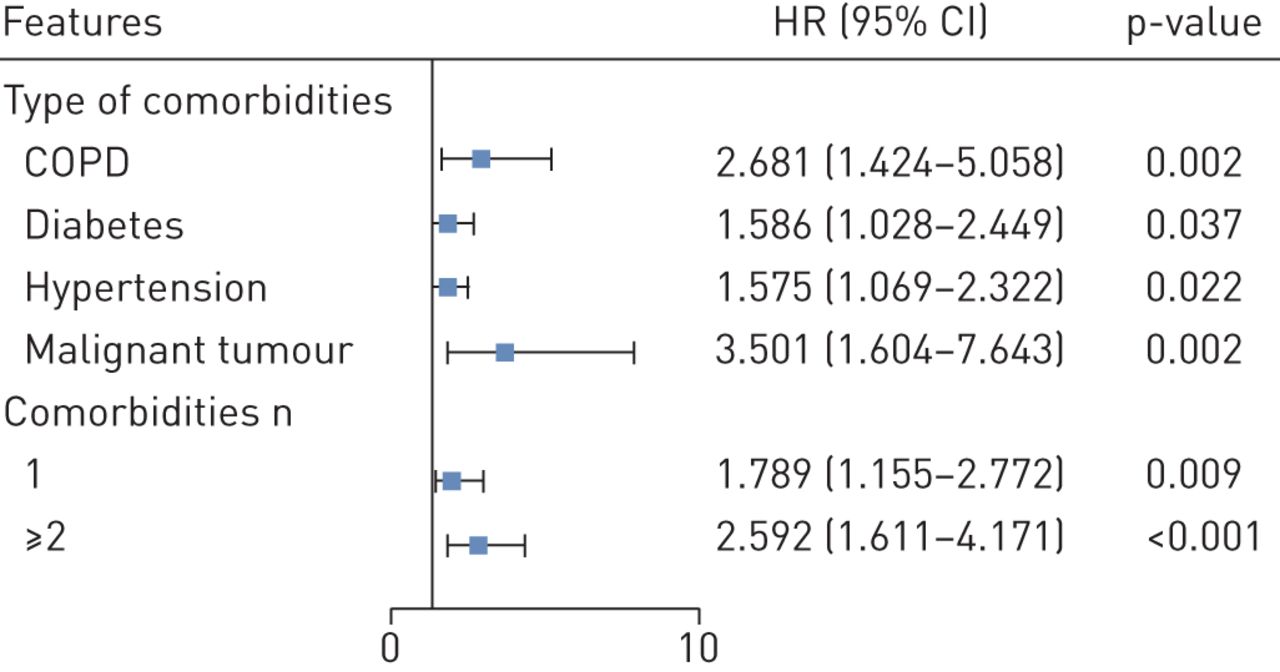
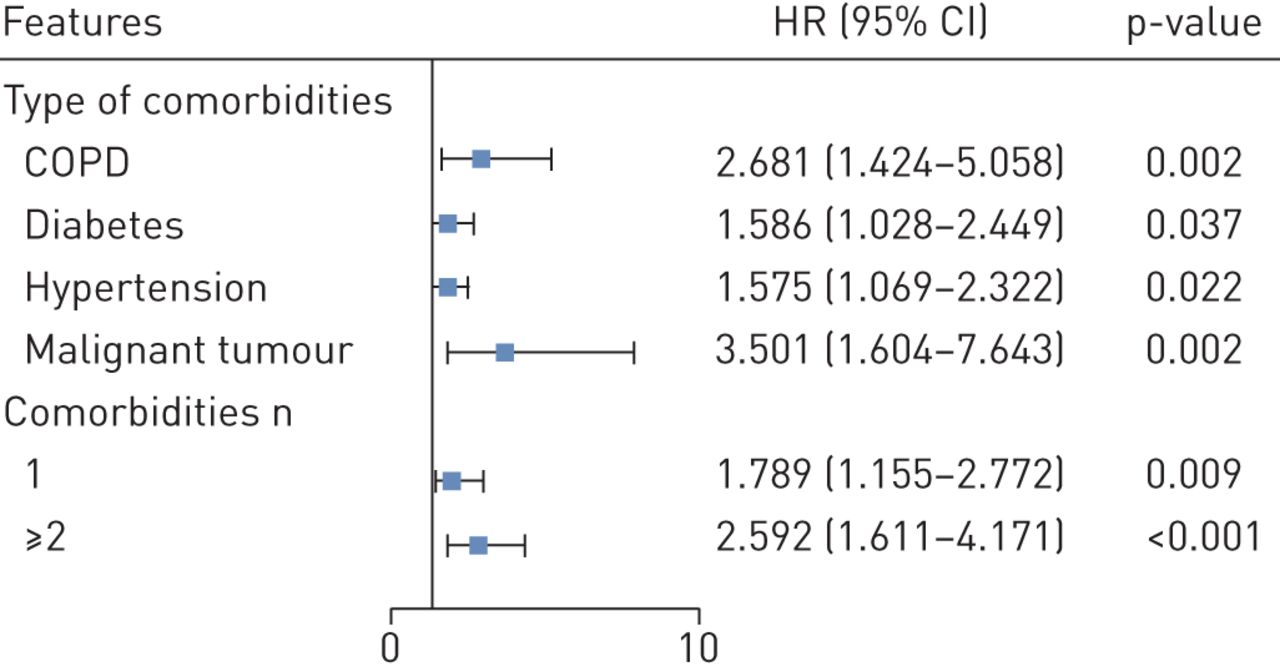
与具有单一合并症的人相比,有两种或更多种可用的合并症的患者对复合终点进行了显着升级的风险,与没有合并症的人(所有P <0.05)(图1)。调整年龄和吸烟状态后,COPD患者(HR(95%CI)2.68(1.42-5.05)),糖尿病(1.59(1.03-2.45)),高血压(1.58(1.07-2.32))和恶性肿瘤(3.50(1.60-7.64))更有可能达到综合端点而不是那些没有(图2)。介绍了未调整分析的结果表E1和E2。总体而言,未经调整和调整分析的结果没有重大改变。与没有合并率的患者相比,HR(95%CI)为1.79(1.16-2.77),患有至少一种合并症和2.59(1.61-4.17)的患者,其中两个或多个合并症(图2)。Subgroup analysis by stratifying patients according to their age (<65 yearsversus≥65 years) did not reveal substantial difference in the strength of associations between the number of comorbidities and mortality of COVID-19 (table E3)。
a)达到或没有任何合并症患者之间的复合端点的时间依赖性风险。b)患者在没有任何合并症的患者之间达到复合终点的时间依赖性风险,单一合并症的患者和两个或多个合并症的患者。施用Cox比例危害回归模型以确定与复合端点相关的潜在风险因素,危险比和95%置信区间报告。
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Predictors of the composite end-points in the proportional hazards model. Hazard ratio (95% confidence interval) are shown for the risk factors associated with the composite end-points (admission to intensive care unit, invasive ventilation or death). The comorbidities were classified according to the organ systems as well as the number. The scale bar indicates the hazard ratio. Cox proportional hazard regression models were applied to determine the potential risk factors associated with the composite end-points, with the hazard ratio (95% confidence interval) being reported. The model has been adjusted with age and smoking status.
讨论
OU.r study is the first nationwide investigation that systematically evaluates the impact of comorbidities on the clinical characteristics and prognosis in patients with COVID-19 in China. Circulatory and endocrine comorbidities were common among patients with COVID-19. Patients with at least one comorbidity, or even more so, were associated with poor clinical outcomes. These findings have provided further objective evidence, with a large sample size and extensive coverage of the geographic regions across China, to take into account baseline comorbid diseases in the comprehensive risk assessment of prognosis among patients with COVID-19 on hospital admission.
总体而言,我们的研究结果已回应最近发表的研究,就Covid-19患者的合并症常见而言[3–7]。尽管由于样本量有限,但患者进行了有限的地区,但是各种研究中的比例有相当多的变化,但循环疾病(包括高血压和冠心病)仍然是最常见的合并症[3–7]。Apart from circulatory diseases, endocrine diseases such as diabetes were also common in patients with COVID-19. Notwithstanding the commonness of circulatory and endocrine comorbidities, patients with COVID-19 rarely reported having comorbid respiratory diseases (particularly COPD). The reasons underlying this observation have been scant, but could have arisen from the lack of awareness and the lack of spirometric testing in community settings that collectively contributed to the under-diagnosis of respiratory diseases [33]。It should be stressed that the observed frequency of comorbidity may also reflect the transmission dynamics within particular age groups, case detection or testing practices or hospital admission policies during the early phases of the epidemic. Consistent with recent reports [3–7], the percentage of patients with comorbid renal disease and malignancy was relatively low. Our findings have therefore added to the existing literature on the spectrum of comorbidities in patients with COVID-19 based on the larger sample sizes and representativeness of the whole patient population in China.
一些现有的文献报告记录了禽流感患者的较差临床结果的升级风险[14–18], SARS-CoV [19] and MERS-CoV infections [20–28]。与预后较差的糖尿病相关的最常见的合并症[25,29],高血压[28], respiratory diseases [19,28], cardiac diseases [19,28],怀孕[16],肾病[28]和恶性肿瘤[19]。我们的研究结果表明,与其他严重的急性呼吸爆发,诸如COPD,糖尿病,高血压和恶性肿瘤等同种性,易患Covid-19患者的不利临床结果。然而,与文献报告相比,不同的合并症与预后之间的关联强度较不一致[16,19,25,28]。例如,心脏病患者的风险和流感,SARS-COV或MERS-COV感染的缺乏临床结果不确定[16,19,25,28]。Except for diabetes, no other comorbidities were identified to be the predictors of poor clinical outcomes in patients with MERS-CoV infections [25]。然而,很少有研究探索了这些协会的基础机制。K.ulscar.et al.[27] showed that MERS-CoV infections resulted in prolonged airway inflammation, immune cell dysfunction and an altered expression profile of inflammatory mediators in diabetic mice models. A network-based analysis indicated that SARS-CoV infections led to immune dysregulation that could help explain the escalated risk of cardiac diseases, bone diseases and malignancy [34]。Therefore, immune dysregulation and prolonged inflammation might be the key drivers of the poor clinical outcomes in patients with COVID-19 but await verification in more mechanistic studies.
它得到了很好的是,一些合并症经常共存。例如,糖尿病[35] and COPD [36]经常与高血压或冠心病共存。因此,共存合并症的患者更有可能具有较差的基线福祉。重要的是,与没有或仅单一合并症的人相比,我们已经验证了两种或更多种可用性的患者预后的显着升级的风险。我们的研究结果暗示,在预测Covid-19患者的预后时,应考虑分类和数量。
OU.r findings suggested that patients with comorbidities had greater disease severity compared with those without. Furthermore, a greater number of comorbidities correlated with greater disease severity of COVID-19. The proper triage of patients should be implemented by carefully inquiring about the medical history because this will help identify patients who would be more likely to develop serious adverse outcomes of COVID-19. Moreover, better protection should be given to the patients with COIVD-19 who had comorbidities upon confirmation of the diagnosis.
主要限制是录取合并症的自我报告。在缺乏意识和缺乏诊断检测中可能源于缺乏意识和/或缺乏诊断检测的情况下,可能导致临床预后的真正强度有助于低估。报告中的合并症也可能导致过度估计与不利结果的关联强度。然而,显着的报告下不太可能因为我们的报告的频谱很大程度上与现有文献一致[3–7] and all patients were subject to a thorough history taking after hospital admission. The relatively low age might help explain the low prevalence of COPD in our cohort. Moreover, the duration of follow-up was relatively short and some patients remained in hospital at the time of writing. More studies that explore the associations in a sufficiently long time-frame are warranted. Caution should be exercised when extrapolating our findings to other countries where there are outbreaks of COVID-19 since the prevalence of comorbidities may differ among different countries. Therefore, future studies that include an external validation of the results would be desirable. Although the temperature and systolic blood pressure differed between some subgroups, they were unlikely to be clinically relevant. Finally, because of the rapid evolving outbreak globally, ongoing studies with the inclusion of more patients would be needed to increase the statistical power and lend support to subgroup analyses stratified by the specific comorbidities (即COPD) and their association with the risk of death.
结论s
在实验室确诊的Covid-19病例中,任何合并症的患者都会产生较差的临床结果。更多的合并症也与较差的临床结果相关。A thorough assessment of comorbidities may help establish risk stratification of patients with COVID-19 upon hospital admission.
Supplementary material
Supplementary Material
Please note:supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary materialERJ-00547-2020.Supplement.
Shareable PDF
Supplementary Material
This one-page PDF can be shared freely online.
Shareable PDFERJ-00547-2020。阿尔摩
Acknowledgement
我们感谢医院工作人员(请参阅附录中supplementary material对于完整列表),他们努力收集信息。我们感谢Zong-jiu Zhang,Ya-Hui Jiao,Bin du,新强高和陶维(国家卫生委员会),玉飞和志岭赵(广东省卫生委员会)的协调,易民李,滋阴梁,nu福张,石悦李,清 - 黄,文西黄,明丽(广州呼吸健康研究院)大大促进了患者数据收集。特别感谢统计团队成员郑陈,董汉,李,郑陈,志莹湛,金健陈,李军徐和萧汉徐(有机体衰竭研究国家重点实验室)南方医科大学公共卫生学院热带病研究中的生物统计学重点实验室。我们还感谢李强王,威鹏蔡和紫盛陈(广州医科大学附属医院),长兴欧,萧敏鹏,锡妮,元王,谅解备忘录,鑫昊,齐华河,景沛李,徐凯李,魏王,李敏,y磊张,景伟刘,新国熊,魏俊华,三梅玉,奔跑- 洞秦,思阳瑶,博梦张,萧宏谢湛洪谢,万迪王,张小贤张,慧尹徐,紫清周,莹江,倪刘,倪刘,京泾元,郑朱,杰霞张,洪浩李,魏华黄,陆林王,李莹李,李芬,嘉博高,蔡辰李,薛 -魏辰,嘉博高,明山薛,寿谢黄,嘉曼堂,魏古和金林王(广州呼吸健康研究院)为竭诚为数据进入和验证。我们很感谢腾讯有限公司为中国在中国录取Covid-19患者提供认证医院的数量。 Finally, we thank all the patients who consented to donate their data for analysis and the medical staff working in the front line.
Footnotes
本文提供了补充材料www.qdcxjkg.com.
Author contributions: Wei-jie Guan, Wen-hua Liang, Jian-xing He, and Nan-shan Zhong participated in study design and study conception; Wen-hua Liang, Yi Zhao, Heng-rui Liang, Zi-sheng Chen, Chun-quan Ou, L. Li, Ping-yan Chen, Jian-fu Li, Cai-chen Li, Li-min Ou, Bo Cheng, Wei Wang and Shan Xiong performed data analysis; Ru-chong Chen, Chun-li Tang, Tao Wang, Ling Sang, Zheng-yi Ni, Jie Xiang, Yu Hu, L. Li, Hong Shan, Chun-liang Lei, Yi-xiang Peng, Li Wei, Yong Liu, Ya-hua Hu, Peng Peng, Jian-ming Wang, Ji-yang Liu, Zhong Chen, Gang Li, Zhi-jian Zheng, Shao-qin Qiu, Jie Luo, Chang-jiang Ye, Shao-yong Zhu, Lin-ling Cheng, Feng Ye, Shi-yue Li, Jin-ping Zheng, Nuo-fu Zhang, and Nan-shan Zhong recruited patients; Wei-jie Guan, Jian-xing He, Wen-hua Liang and Nan-shan Zhong drafted the manuscript; all authors provided critical review of the manuscript and approved the final draft for publication.
支持声明:广东省科学技术系国家卫生委员会支持。该资助者在研究中没有作用。本文的资金信息已存入CrossRef Resder注册表。
Conflict of interest: Wei-jie Guan has nothing to disclose.
Conflict of interest: Wen-hua Liang has nothing to disclose.
利益冲突:易赵没有披露。
Conflict of interest: Heng-rui Liang has nothing to disclose.
兴趣冲突:Zi-Sheng Chen没有什么可披露的。
利益冲突:易民李没有什么可以披露的。
Conflict of interest: Xiao-qing Liu has nothing to disclose.
Conflict of interest: Ru-chong Chen has nothing to disclose.
兴趣冲突:春丽唐没有披露。
利益冲突:陶旺没有什么可以披露的。
利益冲突:春泉欧没有披露。
Conflict of interest: Li has nothing to disclose.
Conflict of interest: Ping-yan Chen has nothing to disclose.
Conflict of interest: Ling Sang has nothing to disclose.
Conflict of interest: Wei Wang has nothing to disclose.
利益冲突:建益李无所事事。
兴趣冲突:蔡辰李没有披露。
兴趣冲突:李敏某没有什么可以披露的。
Conflict of interest: Bo Cheng has nothing to disclose.
Conflict of interest: Shan Xiong has nothing to disclose.
兴趣冲突:郑益尼没有披露。
Conflict of interest: Jie Xiang has nothing to disclose.
Conflict of interest: Yu Hu has nothing to disclose.
利益冲突:雷刘没有什么可以披露的。
利益冲突:洪山没有什么可披露的。
Conflict of interest: Chun-liang Lei has nothing to disclose.
利益冲突:易翔彭没有什么可披露的。
Conflict of interest: Li Wei has nothing to disclose.
利益冲突:永刘无所事事。
Conflict of interest: Ya-hua Hu has nothing to disclose.
Conflict of interest: Peng has nothing to disclose.
Conflict of interest: Jian-ming Wang has nothing to disclose.
兴趣冲突:吉阳刘没有披露。
Conflict of interest: Zhong Chen has nothing to disclose.
Conflict of interest: Gang Li has nothing to disclose.
Conflict of interest: Zhi-jian Zheng has nothing to disclose.
Conflict of interest: Shao-qin Qiu has nothing to disclose.
Conflict of interest: Jie Luo has nothing to disclose.
利益冲突:长江烨无所事事。
兴趣冲突:邵永朱无所事事。
兴趣冲突:林玲成无一想。
Conflict of interest: Feng Ye has nothing to disclose.
Conflict of interest: Shi-yue Li has nothing to disclose.
Conflict of interest: Jin-ping Zheng has nothing to disclose.
利益冲突:Nuo-Fu张没有什么可披露的。
Conflict of interest: Nan-shan Zhong reports grants from the National Health Commission and Dept of Science and Technology of Guangdong Province, during the conduct of the study.
利益冲突:建 - 兴他没有披露。
The version of this article originally published in early view format contained some transcription errors in the total subject numbers presented in table 3. This was an issue that arose in compiling the table and the underlying results and conclusions are not affected by the correction.
- 收到了2020年3月4日。
- AcceptedMarch 13, 2020.
- Copyright ©ERS 2020
此版本在Creative Commons归因非商业许可证4.0的条款下分发。
References