





Abstract
Breath-hold divers employ glossopharyngeal insufflation (GI) in order to prevent the lungs from compressing at great depth and to increase intrapulmonary oxygen stores, thus increasing breath-hold time.
The presented case study shows the physiological data and dynamic magnetic resonance imaging (dMRI) findings of acute hyperinflation, deliberately induced by GI, in a breath-hold diver and discusses the current state of knowledge regarding the associated hazards of this unique competitive sport.
Static and dynamic lung volumes and expiratory flows were within the normal range, with vital capacity and peak expiratory flow being higher than the predicted values. Airway resistance and diffusing capacity of the lung for carbon monoxide were normal. Static compliance was normal and increased five-fold with hyperinflation. dMRI revealed a preserved shape of the thorax and diaphragm with hyperinflation. A herniation of the lung beneath the sternum and enlargement of the costodiaphragmatic angle were additional findings during the GI manoeuvre. After expiration, complete resolution to baseline was demonstrated.
Hyperinflation can be physiological and even protective under abnormal physical conditions in the sense of acute adaptation to deep breath-hold diving. Dynamic magnetic resonance imaging is adequate for visualisation of the sequence of the glossopharyngeal insufflation manoeuvre and the complete reversibility of deliberate hyperinflation.
- Breath-hold diving
- dynamic magnetic resonance imaging
- glossopharyngeal insufflation
- hyperinflation
- lung
肺恶性通货膨胀是一个慢性obstr的标志uctive pulmonary disease. Hyperinflation is caused by inflammatory changes to the lung parenchyma that result in decreased elasticity. Functionally, hyperinflation implies an increased ratio of residual volume (RV) to total lung capacity (TLC), with a shift of tidal breathing at the expense of inspiratory capacity. Flattening of the diaphragm, sternal bowing, chest kyphosis and enlarged intercostal spaces, resulting in a barrel chest, are typical radiological findings1. Extremes of lung physiology, however, may radiologically imitate conditions that, in a chronic situation, indicate a pathological status.
CASE REPORT
A 42-yr-old male who presented for a medical check-up had a history of competitive breath-hold diving employing glossopharyngeal insufflation (GI) breathing, a technique that deliberately causes hyperinflation of the lung. The physiological data and dynamic magnetic resonance imaging (dMRI) findings of this case of acute deliberately induced lung hyperinflation are presented and the current state of knowledge regarding the associated hazards of this unique competitive sport are discussed.
Assessment
Clinical data
Clinical examination revealed a 42-yr-old healthy athletic nonsmoker (height 185 cm and weight 84 kg), with normal cardiopulmonary status. He had been performing breath-hold diving for a number of years and held a national record in a competitive discipline. His personal best static apnoea performance,i.e.breath-holding for as long as possible with the respiratory tract immersed, was >6 min.
Physiological parameters of the diver
The pulmonary function testing before magnetic resonance imaging (MRI) included forced, body plethysmography and measurement of the diffusing capacity of the lung for carbon monoxide at rest. Static and dynamic lung volumes and expiratory flows were within the normal range, with the vital capacity (VC) and peak expiratory flow being higher than the predicted values2. Airway resistance and diffusing capacity were normal (table 1⇓). A dMRI imaging sequence showing the diver performing spirometry in comparison to a patient with emphysema is available in the online supplementary material.
Pulmonary function data of the breath-hold diver
For assessment of static compliance, the expiratory pressure/volume curve over the range 60–90% TLC was measured. The regular static compliance of the diver was 3.9 L·kPa−1, which increased after hyperinflation to 21.2 L·kPa−1(fig. 1⇓).
Pressure/volume curve of the diver a) at rest and b) after glossopharyngeal insufflation (GI). The increased slope of the curve after the GI manoeuvre is of note (·······: line of best fit). The regular static compliance was 3.9 L·kPa−1and 21.2 L·kPa−1after hyperinflation.Ptp: transpulmonary pressure.
Imaging modalities
The diver underwent morphological MRI and dMRI using a 1.5-T MRI scanner (Avanto; Siemens Medical Solutions, Erlangen, Germany) after giving informed consent and according to the ethical guidelines of the institutional review board. A half-Fourier acquisition single-shot turbo spin-echo sequence was used for morphological evaluation, revealing a normally shaped chest wall with a well-preserved diaphragmatic dome.
For visualisation of the forced expiratory manoeuvre, dMRI was performed using a two-dimensional fast, low angle shot pulse sequence with 10 images·s−1.
Glossopharyngeal inhalation manoeuvre
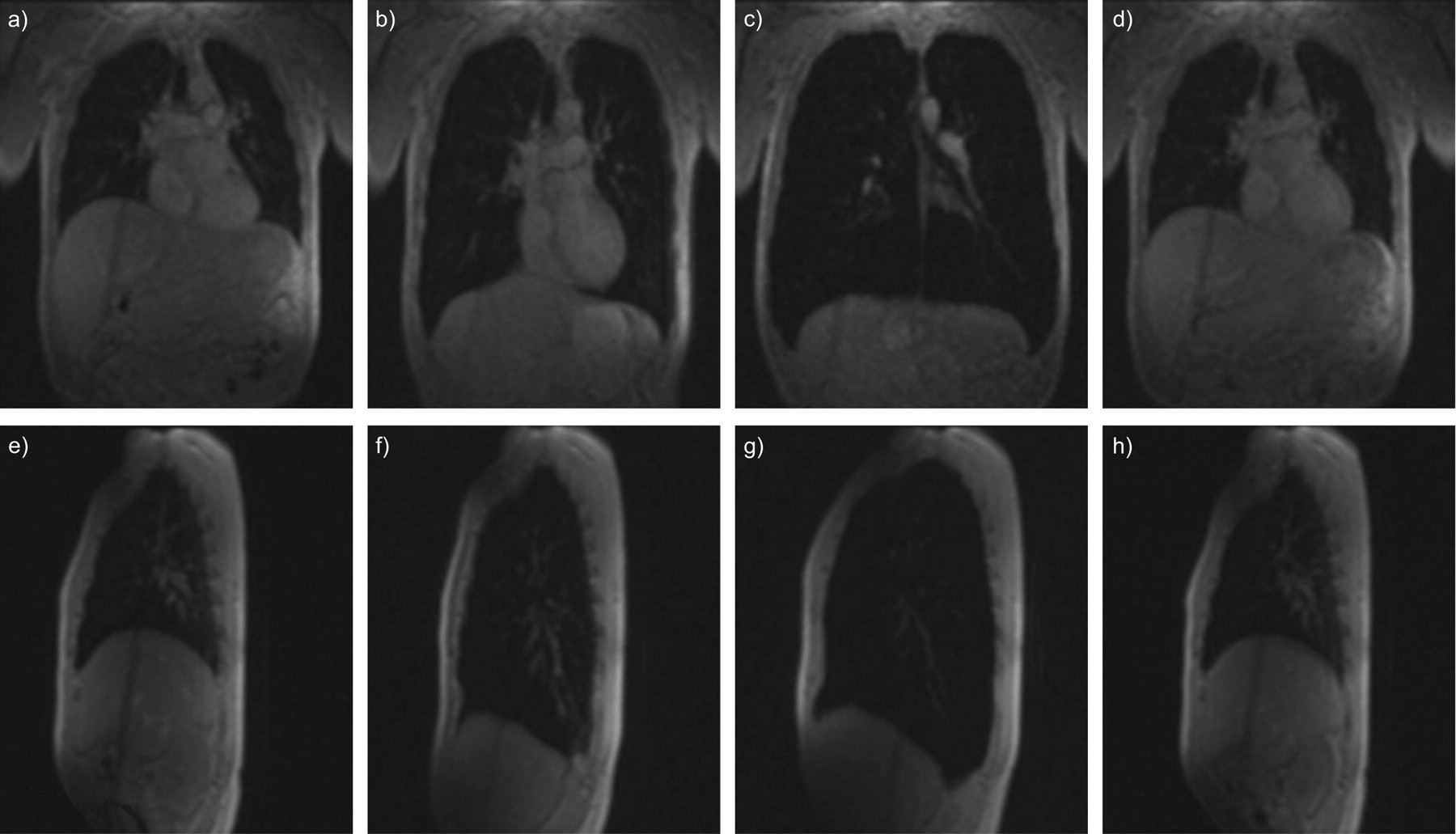
After deep inhalation to TLC, the diver forced mouthfuls of air into the lungs, opening the glottis just for the GI manoeuvre. The manoeuvre was assed by dMRI (fig. 2⇓) and simultaneously monitored spirometrically using a magnetic resonance-compatible spirometer (fig. 3⇓)3. The measured increase in intrathoracic gas volume amounted to 2.6 L (table 1⇑).
潜水员pe的动态磁共振成像rforming the glossopharyngeal insufflation (GI) manoeuvre: a–d) coronal view and e–h) sagittal view, starting from forced residual capacity (FRC; a and e). Of note is the bilateral symmetrical hyperinflation of the thorax from total lung capacity (b and f) to deliberate maximal hyperinflation due to GI (c and g), with maximal dorsoventral extension of the chest wall, downward movement of the diaphragm with a well-preserved dome shape (c), herniation of the lung beneath the xyphoid and enlargement of the dorsal costodiaphragmatic recessus (g). This all resolved to FRC level at baseline after expiration (d and h).
Magnetic resonance-compatible spirometric curve showing the glossopharyngeal insufflation manoeuvre. After a deep expiration, the diver inhaled to vital capacity (VC) and performed buccal pumping, which is not recorded spirometrically (------). Owing to the increased intrathoracic volume, expiratory VC exceeds inspiratory VC by 2.6 L.
The increase in lung volume shown spirometrically is demonstrated clearly not only by increases in the apicodiaphragmatic, lateral and anteroposterior lengths but also by enlargement of the costodiaphragmatic angle and subxyphoid herniation of the lung. Following expiration, the chest wall and diaphragm returned to the initial level of forced residual capacity.
Management
The diver is continuing to train these extreme manoeuvres without any pulmonary complication at present, or any change in lung function.
DISCUSSION
Glossopharyngeal breathing was first described in 1951 in patients with post-poliomyelitic syndrome4. In these patients with pronounced impairment of the respiratory muscles and consequently a very low VC, the technique permitted an increase in VC, thereby prolonging the off-respirator time. Later, this technique was reported to be effective in a larger cohort of patients with post-polio syndrome5, rapid progressive tetraparesis6or Duchenne muscular dystrophy7. Only recently has it been reported that breath-hold divers also employ this technique8. After filling the lungs to TLC, a mouthful of air is compressed by the oropharyngeal muscles and then forced into the lungs. This insufflation manoeuvre is repeated several times until a sensation of fullness occurs. The glottis is closed after each insufflation. For athletes competing with regard to breath-hold time, depth or distance, this deliberate hyperinflation is helpful in many respects. First, the athletes need to draw air from the lungs into the pharynx in order to equalise middle-ear pressures when going down. Secondly, by filling the lungs with additional air, the available pulmonary oxygen store is increased. In the particular example of the present diver, the additional 2.59 L contain ∼543 mL oxygen, thus enabling him to extend his breath-hold duration by up to 2 min beyond normal, depending on his metabolic rate. Thirdly, lung squeeze may occur in circumstances under which the total lung volume is compressed with increasing depth,i.e.increasing water pressure, beyond the RV8. Predictions of the maximal achievable depth are based on the theory of Boyle's Law (P1V1 = P2V2assuming constant temperature). For example, without consideration of blood redistribution, the present diver’s depth limit is 6.1 atmospheres (TLC/RV = 8.6 L/1.4 L),i.e.∼50 m of seawater. He was able to reach a personal depth record of 50 m. Thus the use of GI permits breath-hold divers to reach, and in some situations to exceed, the depth limits set by their individual TLC/RV ratio. Indeed, the more recent depth records have well surpassed previous predictions based on theory not taking GI into account9,10.
GI exerts considerable mechanical stress on lung elastic properties. Increases in intrapulmonary and transpulmonary pressures up to 109 and 80 cmH2O, respectively, have recently been measured following GI11. Obviously, the lungs of elite breath-hold divers withstand transpulmonary pressures and volumes far greater than those to which lungs would normally be exposed.
The current MRI investigation concurs with the evidence from the functional assessment of extreme overdistension of the respiratory system during GI. To the present authors’ knowledge, this is the first report of MRI being performed while simultaneously controlling for the increase in total lung volume using spirometry. The shape of the thorax was primarily preserved in the diver, although total lung volume, as measured by magnetic resonance-compatible spirometry, increased markedly. Furthermore, the herniation of the lung beneath the sternum and enlargement of the costodiaphragmatic angle demonstrate the distensibility and high performance of trained lungs (fig. 2⇑). In contrast to static MRI12, dMRI can visualise the sequence of the diaphragm and chest wall during the course of the manoeuvre and demonstrate the resolution to baseline following expiration. Whether the unusual distensibility of breath-hold divers’ lungs can be explained as an effect of structural adaptation to repeated lung extension or by an unusual genetic background remains to be elucidated. However, one case of asymptomatic pneumomediastinum has been reported from computed tomographic assessment of a breath-hold diver who increased the volume of gas in his lungs by ∼1 L beyond his TLC13. Thus this complication may occur more frequently than reported.
There are serious risks associated with breath-hold diving. The oxygen stores of the lungs and blood are depleted until the partial pressure of oxygen in the brain may become so low that the diver risks loss of consciousness,i.e.drowning. Loss of motor control (defined as the presence of hypoxic signs first appearing after surfacing without complete loss of consciousness) is reported to occur in up to 10% of divers during breath-hold competitions14. In addition, cases of haemoptysis following breath-hold dives have been reported15–17. Rupture of the alveolocapillary membrane may be caused by elevation of the pulmonary transcapillary wall pressure due to decreases in intrathoracic pressure when total lung volume at depth approaches RV16. Apart from these acute hazards, there is scanty information regarding possible long-term risks. One investigation postulated from ECG measurements that competitive breath-hold diving may carry an increased cardiopulmonary risk18. However, these findings need to be confirmed by longitudinal studies of the cardiopulmonary system of competitive breath-hold divers.
In conclusion, the present investigation demonstrates that lung hyperinflation induced by deliberate glossopharyngeal insufflation may grossly imitate the hyperinflation seen in chronic obstructive pulmonary disease patients. This hyperinflation, however, is fully reversible and even protective in the sense of an acute adaptation to an environmental challenge such as deep breath-hold diving.
Statement of interest
None declared.
Footnotes
This article has a supplementary material video accessible fromwww.www.qdcxjkg.com
- ReceivedSeptember 7, 2007.
- AcceptedJanuary 30, 2008.
- © ERS Journals Ltd











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}