





Case history
A 26‐yr-old male patient was referred to the outpatient clinic with a history of recurrent respiratory infections since 8 yrs of age and a daily productive cough with purulent sputum. He related nasal sneezing, hoarseness and wheezing episodes to weather changes and exposure to dusts andchemicals. Dyspnoea on exertion was present during exacerbations. He had never smoked and denied any family history of respiratory disease. Physical examination was unremarkable.
胸部X光片(图1×和2×) and later a high-resolution computed tomography (HRCT) of the chest (figs 3×和4×) were ordered. Pulmonary function tests showed a forced vital capacity (FVC) of 3.16 L (66% of predicted), a forced expiratory volume in one second (FEV1)2.21 L(55%PRED),FEV1/FVC of 0.70 (83% pred) and a forced mid‐expiratory flow of 1.51 (33% pred). There was no response to bronchodilator.
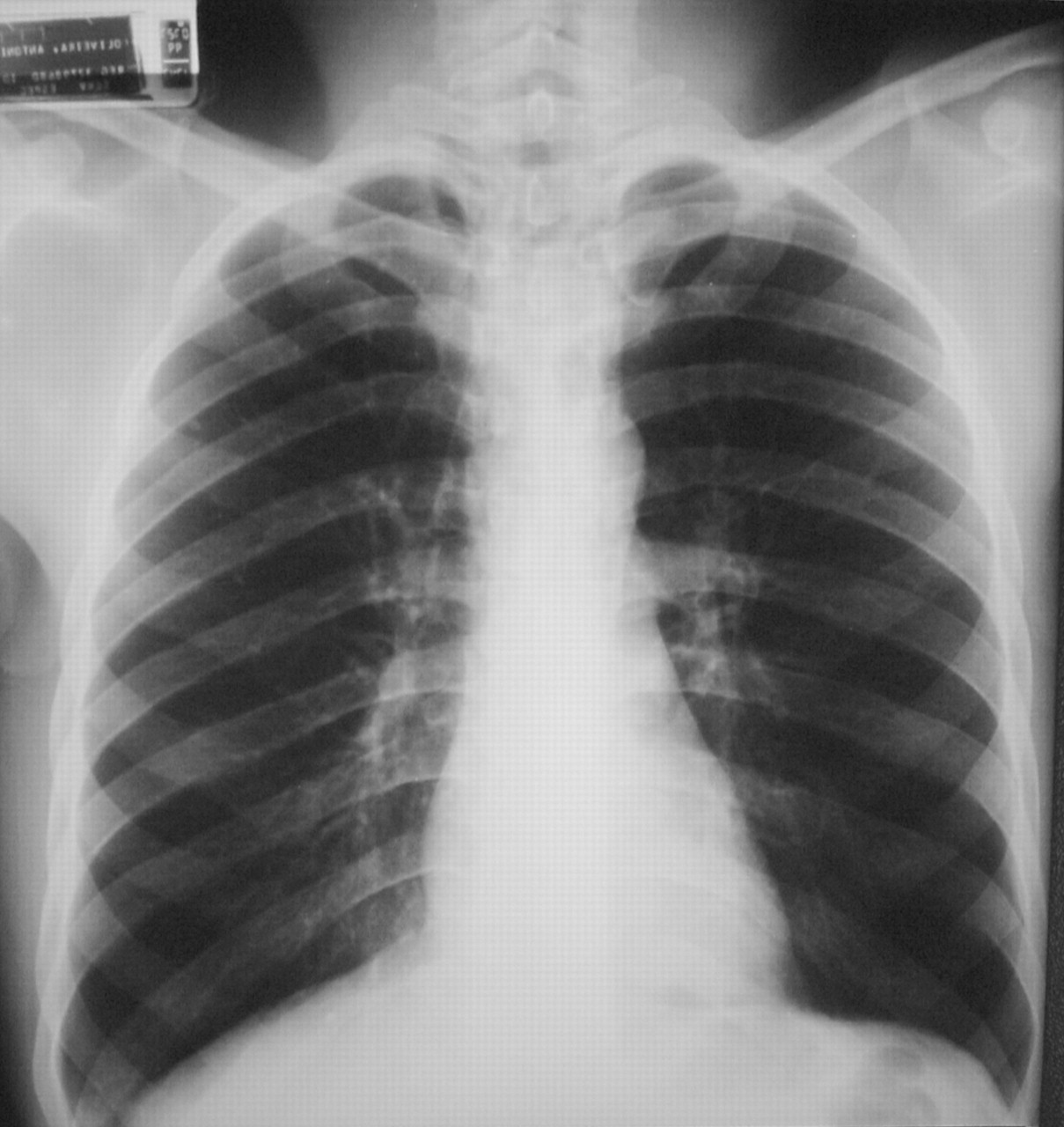
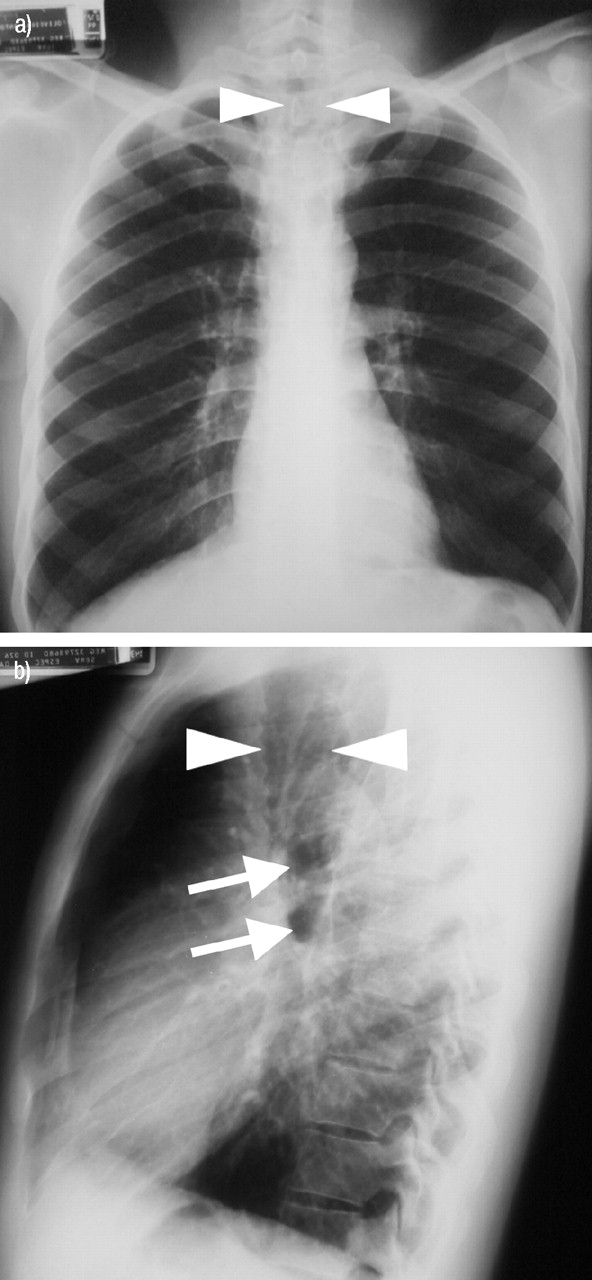
后胸部roentgen图。
侧胸部roentgon图。
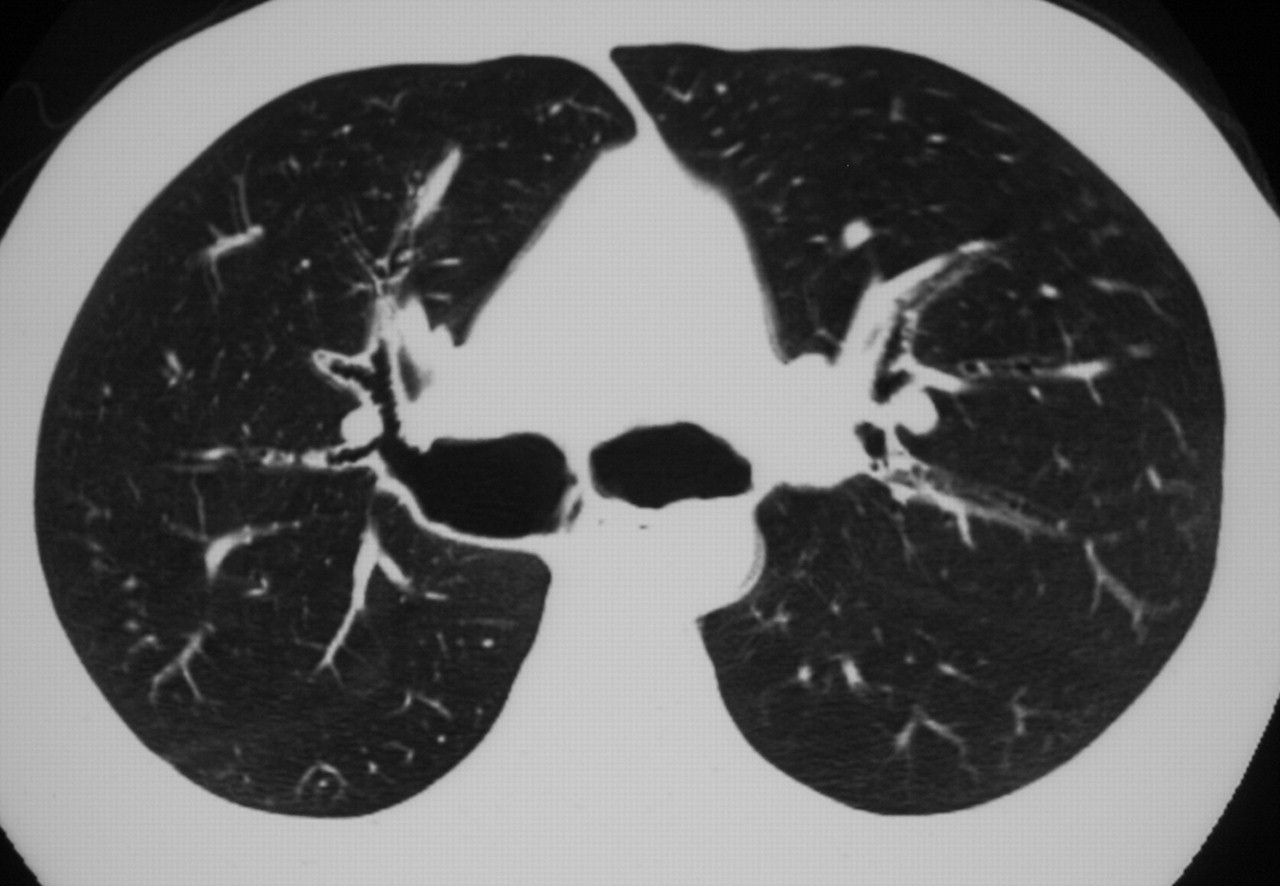
胸部的高分辨率计算机断层扫描。

胸部的高分辨率计算机断层扫描。
在翻页之前,请解释X光片和历史记录,并提出可能的诊断。
Interpretation of the radiographical exams and pulmonary function tests
胸部X光片揭示了气管和主茎支气管的扩大,最好在外侧膜上看到。HRCT扫描显示出明显肿胀的气管和主茎支气管(气管3.5×3.0 cm;右主支气管3.0×3.0 cm;左主支气管2.5×2.0 cm),远处三分之一的憩室。
Pulmonary function tests reveal a moderate obstructive pattern with no response to bronchodilator.
放大的气管和主要支气管被突出显示为5×分别通过箭头和箭头。图6中的箭头突出显示了憩室×.
箭头显示放大的气管和箭头显示左和右主支气管(分别为上和下箭头)。a)后视图和b)侧视图。

箭头显示气管憩室。
Diagnosis: “Tracheobronchomegaly (Mounier-Kuhn syndrome)”
治疗和临床课程
The patient was referred to long‐term pulmonary physical therapy. He received three courses of antibiotics to treat exacerbations in the last 24 months.
Discussion
气管异藻瘤是Mounier-Kuhn首先描述的一种罕见疾病1in 1932. It is characterised by marked tracheobronchial dilatation and recurrent lower respiratory tract infections.
病因尚不清楚,但已经报道了气管和主支气管的弹性和肌肉组织。结果,一些患者可能会通过气管环出现粘膜疝,从而导致气管憩室。支气管扩张也是综合征的共同特征1–5.
The syndrome is slightly more common in males, usually in their third and fourth decades of life, although some cases have been reported in ages ranging from 18 months to 76 yrs3–5.
Patients with tracheobronchomegaly may have few or no symptoms without any evidence of disease progression. However, some may have symptoms that are largely indistinguishable from bronchiectasis and chronic bronchitis: productive cough, copious purulent sputum, occasional haemoptysis andprogressive dyspnoea, leading to respiratory failure as thelungs become progressively more damaged. Other possible complications include pneumonia, spontaneous pneumothorax, massive haemoptysis and finger clubbing4.
通常可以通过胸部X光片检测到气管直径的增加,尽管如果不寻找它,则可能会错过。喜马拉尔斯坦和加拉格尔2performed an autopsy study in which the diameters of trachea and main stem bronchi of 100 males with no tracheobronchial abnormality were measured. Based on this study, tracheobronchomegaly may be diagnosed when the diameters of the trachea and right and left main bronchus exceeds 3.0 cm, 2.4 cm and 2.3 cm, respectively. This can be best measured by HRCT. Pulmonary function tests may reveal an obstructive pattern with increased residual volume and total lung capacity.
没有针对无症状的气管体肿大患者的具体疗法。必须提供戒烟建议。治疗仅限于在急性加重,物理疗法和姿势排水期间进行强化抗菌治疗,以帮助清除分泌物。手术由于疾病的扩散性而没有价值。使用traquobronchial假体(例如UltraFlex prosthesis; Boston Scientific, Boston, MA, USA) has been reported with good results and may have a role in advanced cases6.
Mounier-Kunh syndrome should always be suspected in a patient with recurrent respiratory infections and chronic sputum production. A careful analysis of the central airways at the chest radiograph of these patients is obligatory.
- 已收到2003年1月8日。
- AcceptedApril 14, 2003.
- ©ERS Journals Ltd







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}