Article Text

Abstract
IntroductionChronic lung disease, often characterised by rapid decline in lung function, is associated with vascular endothelial dysfunction (characterised by moderate to severe excess urinary albumin excretion (eUAE) but their longitudinal relationship is inadequately studied. In a bidirectional longitudinal examination of healthy adults, we analysed the following two hypotheses: (1) rapid decline (ie, highest tertile of lung function decline) predicts eUAE and (2) eUAE predicts rapid decline.
MethodsWe performed a secondary data analysis from 3052 eligible participants from the Coronary Artery Risk Development in Young Adults (CARDIA) study. For analysis 1, the predictor was rapid decline in lung function between the peak value (attained at or before CARDIA visit year 10 or Y10 at a mean age of 35 years) and Y20; and the outcome was incident eUAE at Y20 and/or Y25. For analysis 2, the predictor was eUAE at Y10 and the outcome was rapid decline between Y10 and Y20.
ResultsAfter adjustment for covariates in analysis 1, rapid decline in FEV1or FVC between peak and Y20 predicted incident eUAE at Y20 and/or Y25 (OR 1.51 and 1.44, respectively; p≤0.05 for both analyses). In analysis 2, eUAE at Y10 did not predict subsequent rapid decline.
ConclusionsHealthy adults with rapid decline in lung function are at risk for developing vascular endothelial dysfunction, as assessed by incident eUAE, later in life.
- clinical epidemiology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See:http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
Multiple cross-sectional studies have established an association between chronic lung disease and excess urinary albumin excretion, a marker for vascular endothelial function. This longitudinal study addresses the direction of this association.
Rapid decline in lung function, but still largely within the normal range of absolute lung function, can be used in healthy adults to predict future risk for vascular endothelial dysfunction, as assessed by incident excess urinary albumin excretion.
Serial measurement of rapid decline in lung function can be used in healthy individuals to predict future risk for vascular endothelial dysfunction, as assessed by incident excess urinary albumin excretion.
Introduction
Millions of people worldwide are affected by chronic respiratory diseases, including 64 million people with chronic obstructive pulmonary disease (COPD) which is also the third leading cause of death globally and in the USA.1 2Chronic lung disease, often characterised by rapid decline in lung function and often associated with vascular disorders,3is cross-sectionally associated with excess urinary albumin excretion (eUAE).4eUAE, a term that encompasses previously used terms of microalbuminuria and macroalbuminuria, is commonly associated with diabetes mellitus, hypertension and ageing. eUAE predicts chronic kidney disease, adverse cardiovascular outcomes and death.5eUAE起源于增加白蛋白t的泄漏hrough the glomerular filtration barrier. This filtration barrier comprises a fenestrated glomerular epithelium consisting of podocytes and glycocalyx, the latter also protects the endothelium against atherosclerosis. This filtration barrier is injured by systemic inflammation and oxidant stress, manifesting as eUAE. In addition to the renovascular bed, eUAE is a marker for endothelial dysfunction that affects the cardiovascular bed.6
Our study objective was to examine the association between rapid decline in lung function (a marker for chronic lung disease) and eUAE (a marker for renovascular and cardiovascular endothelial dysfunction) in healthy adults. If eUAE predicts lung function decline in healthy subjects, interventions based on improving vascular endothelial function may help prevent and treat chronic lung disease. On the other hand, if lung function decline predicts eUAE in healthy adults, the former can serve as a novel preclinical marker for future vascular disease. Further, cardiovascular or renovascular disease may be preventable and treatable using interventions that either improve lung health or target common mediatory pathways. In a bidirectional longitudinal examination of healthy young adults, we hypothesised in our first analysis that rapid lung function decline predicts eUAE. In our second analysis, we reversed the temporal association and hypothesised that eUAE predicts rapid decline. To help achieve our objective, we analysed the national Coronary Artery Risk Development in Young Adults (CARDIA) dataset. With data collected over 25 years, the CARDIA study provides a unique opportunity to analyse longitudinal changes in both lung function and eUAE.
Methods
We performed a longitudinal secondary analysis of data from the CARDIA study that is designed to study development of heart disease in healthy adults. Since 1985, the CARDIA study has been collecting data using interviewer-administered and self-administered questionnaires, spirometry and laboratory test results from 5115 randomly selected participants from Birmingham, Alabama, Chicago, Illinois, Oakland, California, and Minneapolis, Minnesota. The participation response rate at the start of the study was approximately 50%. At the time of recruitment, the participants were balanced on race (52% blacks, 48% white) and sex (54% female, 46% male), as well as educational attainment and age distribution (within the age range of 18–30 years). After their initial examination, the participants were asked to follow-up at CARDIA examination visit years 2 (Y2), Y5, Y7, Y10, Y15, Y20 and Y25. The follow-up rates for the survivors at these visits were 91%, 86%, 81%, 79%, 74%, 72% and 72%, respectively. IRB approval was obtained by the CARDIA study and all individual study sites. Written and signed informed consent was obtained from each participant at each examination. Additional details on the CARDIA study have been published previously.7
Inclusion and exclusion criteria
We excluded all participants with self-reported physician diagnoses of chronic bronchitis (n=106), emphysema (n=8) or kidney disease (n=382) at the CARDIA Y0 visit at a mean age of 25 years in order to focus on healthy young and middle-aged adults. Also excluded were those lost to follow-up after Y0 visit (n=198), those with missing data on spirometry over CARDIA Y0–Y20 such that lung function decline could not be computed (n=1338), those with missing data on urine albumin creatinine ratio at Y20 and/or Y25 (n=28) and two participants who underwent sex change (figure 2).
Predictor and outcome variables
For the first analysis, the primary outcome was incident eUAE, defined as the new occurrence of moderate to severe eUAE at CARDIA Y20 and/or Y25 examination visits at a mean age of 45 and/or 50 years (without antecedent excretion). Moderate eUAE or A2 category of albuminuria,8previously termed microalbuminuria, was defined by 25–300 mg of albumin/g of urine creatinine. Severe eUAE or A3 category of albuminuria,8previously termed macroalbuminuria, was defined by >300 mg of albumin/g of urine creatinine (Table E-V in the online supplementary material. This variable was measured by the laboratory analysis of albumin and creatinine in ‘spot’ urine specimens and by calculating the ratio of their values at Y10, Y20 and Y25. Albumin was assessed using a nephelometric procedure with a specific antialbumin monoclonal antibody, and creatinine was assessed using the Jaffe method. Albumin excretion rate was corrected using the formula albumin/(ĸ × creatinine), where ĸ adjusts for published race and sex differences in typical daily creatinine excretion, as discussed in theonline supplementary material.9
Alternative outcomes included prevalent eUAE and persistent eUAE. Prevalent eUAE was defined as the occurrence of moderate to severe eUAE at Y20 and/or Y25, irrespective of antecedent excretion. Persistent eUAE was defined by the presence of moderate to severe excess excretion at Y25 plus antecedent excretion on at least one more measurement at Y10, Y15 or Y20 visits.
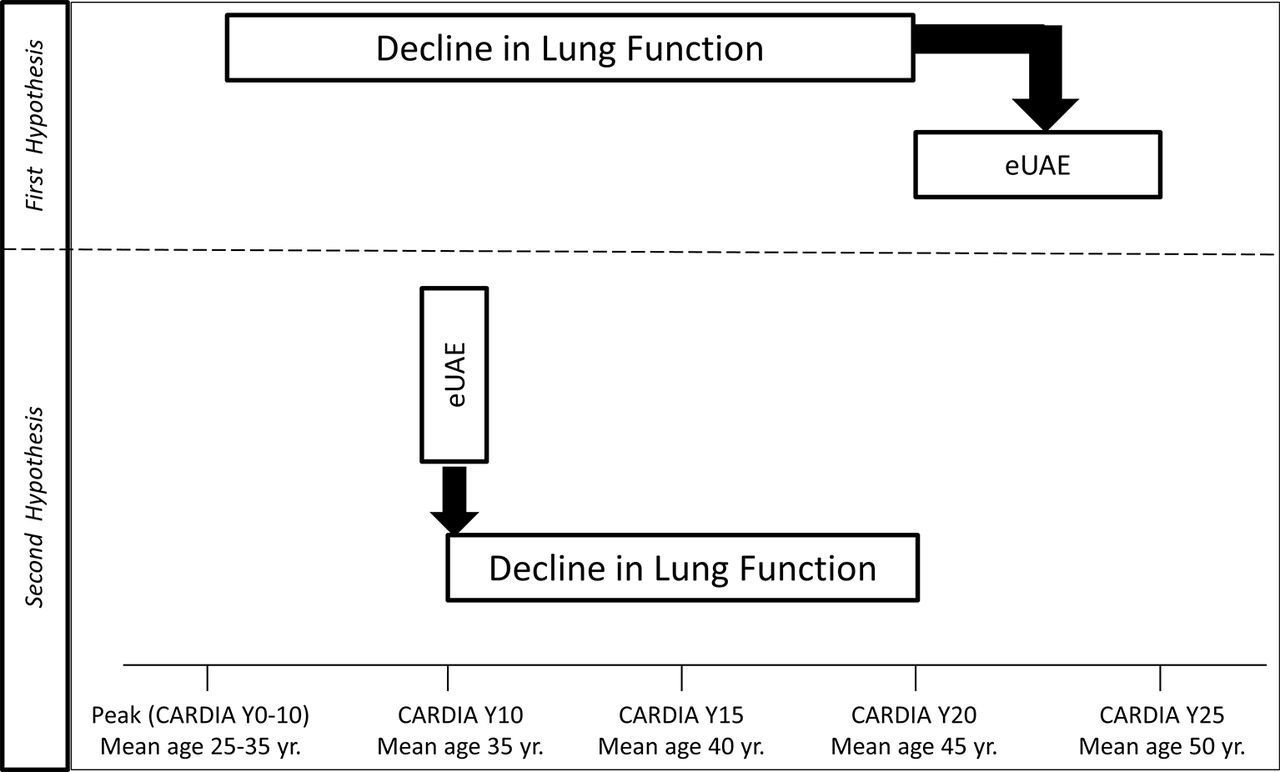
For the first analysis, the predictor was rapid decline in lung function, as assessed between the peak value (determined from the highest FVC or FEV1value at CARDIA Y0, Y2, Y5 and Y10) and Y20 (figure 1).Peak lung function was used rather than Y5 lung function because some participants reached peak lung function before and after Y5. The percentage of participants whose FEV1见顶之前日元是36.1%,after Y5 was 41.4% and at Y5 was 22.5%. Prebronchodilator spirometry was obtained at these visits using a Collins Survey 8- L water sealed spirometer and an Eagle II Microprocessor (Warren E. Collins, Braintree, Massachusetts, USA). CARDIA Y20 lung function was measured using a dry rolling-seal volume OMI spirometer (Viasys, Loma Linda, California, USA). Standard procedures of the American Thoracic Society were followed at all visits.10A detailed description of the testing procedures used during different times was published previously.11
Rapid decline in FEV1and FVC was defined by an annualised decline of ≥52 mL/year and of ≥45.8 mL/year, respectively, between CARDIA peak value and Y20. This definition of rapid decline used the cut point between the highest tertile and the two lower tertiles of decline, established after visually examining the non-linear relationship between decline in lung function and incident eUAE. In additional sensitivity analyses, rapid decline was also examined as a continuous variable.
For the second analysis, our predictor was prevalent eUAE at Y10 and outcome was rapid decline in FVC or FEV1between CARDIA Y10 and Y20, as defined above (figure 1).

Overview of the bidirectional study plan (X depicts time of measurement for the variable). Age refers to the mean age of the study population at the time of the Coronary Artery Risk Development in Young Adults (CARDIA) examination visit year. eUAE, excess urinary albumin excretion.
Covariates
Several covariates were considered, most associated with vascular endothelial function.12 13Standard covariates measured at CARDIA Y5 visit included sex, age, race, height, enlarged waist circumference, diabetes mellitus, current smoking status, pack-years of smoking and physical activity. Additional covariates included hypertension which was measured at either Y0, Y2, Y5, Y7 or Y10 visits; change in body mass index (BMI) which was measured between Y0 and Y5 visits; and peak FEV1or FVC determined from the highest FVC or FEV1value at or before CARDIA Y10 visit. Standard covariates at Y5 visit were selected since Y5 was the median time to attaining peak lung function value in the CARDIA study; the peak lung function value marked the beginning of the measured decline in lung function for studying Hypothesis 1.
Sociodemographic data (age, sex and race) were collected by questionnaire. Self-reported physical activity in the past one year was defined on a five-point Likert scale. High level of activity was defined as more than moderately active, that is, 4 and 5 on the five-point Likert scale. Smoking status was classified as current, former or never-smoker. Height (in cm) without shoes was measured using a vertical ruler; weight (in kg) in light clothing was measured using a calibrated balance beam scale; BMI (in kg/m2) was calculated and change in BMI was defined as ≥10% increase or decrease in value between Y0 and Y5.14Systemic hypertension was defined as systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg or taking antihypertensive medication at that examination visit. Diabetes mellitus was assessed in response to the question, ‘Has a doctor or nurse ever said you had diabetes (high sugar in the blood or urine)?’ Enlarged waist circumference was defined as >102 cm in men and >88 cm in women.
Statistical analysis
The statistical analysis involved χ2and Student's t-test for univariate analysis for categorical and continuous outcomes, respectively. Logistic regression was used for binary outcomes in unadjusted and multivariable models using SAS software V.9.4 and p values <0.05 were considered statistically significant.
Results
Demographic characteristics
Among the 5115 original participants at Y0 visit in the CARDIA cohort, 3052 and 2614 eligible subjects were included for the first and second analyses, respectively (figure 2).Subjects with incident eUAE at Y20 or Y25 had greater prior values of adiposity (ie, greater levels of BMI, change in BMI and waist circumference); greater likelihood of having systemic hypertension, being black and being less physically active; and had lower mean absolute FVC and FEV1values, than those without eUAE (table 1).Subjects with rapid decline between CARDIA peak and Y20 visit also had greater prior values of adiposity (ie, greater levels of BMI, change in BMI and waist circumference); greater likelihood of having systemic hypertension, being older, male and current smokers; and had greater urinary albumin creatinine ratio at Y10 than those without rapid decline (table 2).
Characteristics of study participants at Coronary Artery Risk Development in Young Adults (CARDIA) Y5 examination visit (at a mean age of 30 years), stratified by the presence of incident excess urinary albumin excretion (eUAE) at Y20 or Y25 examination visits (at a mean age of 45 or 50 years)
Characteristics of study participants at Coronary Artery Risk Development in Young Adults (CARDIA) Y5 examination visit (at a mean age of 30 years), stratified by rapid lung function decline (between CARDIA Y20 and peak determined from the highest value at Y0, Y2, Y5 and Y10 visits)
Strengthening the Reporting of Observational Studies in Epidemiology chart for the temporal sequence of analyses. In the first analysis, the predictor was rapid decline in lung function between the peak value (attained at or before Coronary Artery Risk Development in Young Adults (CARDIA) visit year 10 or Y10) and Y20; and the outcome was incident excess urinary albumin excretion (eUAE) at Y20 and/or Y25. For the second analysis, the predictor was eUAE at Y10 and the outcome was rapid decline between Y10 and Y20.
Rapid decline in lung function in young to mid adulthood predicts incident eUAE later in life
Rapid decline in FEV1between CARDIA peak and Y20 visit predicted incident, prevalent and persistent eUAE at Y20 and/or Y25 (table 2; unadjusted p≤0.006 for all analyses). Similar results were obtained with rapid decline in FVC as the predictor variable (table 2andonline supplementary tables E-I, E-II and E-VI).On the other hand, rapid decline in FEV1/FVC ratio (ie, ≥0.89% per year, similarly defined by the cut point between the highest tertile and the two lower tertiles) did not predict incident eUAE (OR 1.13, 95% CI 0.87 to 1.48, p=0.36).
The associations of incident eUAE with rapid FEV1decline remained significant when studying lung function decline as a continuous predictor variable (online supplementary table E-I).The association of incident, prevalent or persistent eUAE with rapid FEV1or FVC decline remained significant after adjustment for covariates (table 3).
Unadjusted analyses of the association between rapid decline in lung function as the predictor variable (between Coronary Artery Risk Development in Young Adults (CARDIA) Y20 and peak determined from the highest value at Y0, Y2, Y5 and Y10 visits) and incident, prevalent and persistent excess urinary albumin excretion (eUAE) as outcome variables (latter measured at Y20 and/or Y25 examination visits at a mean age of 45 and/or 50 years))
eUAE in young adulthood does not predict rapid decline in lung function later in life
In the second analysis, categorically defined prevalent eUAE at CARDIA Y10 did not predict rapid decline in either FVC or FEV1over the subsequent 10-year time period (table 4).当尿白蛋白肌酐比率是里边的ad studied as a continuous independent variable, it did predict subsequent rapid decline in FEV1in univariate analysis (p=0.04) (table 4, footnote 1) but not in multivariable analyses.
Association between rapid decline in lung function† as the predictor variable (between Coronary Artery Risk Development in Young Adults (CARDIA) Y20 and peak determined from the highest value at Y0, Y2, Y5 and Y10 visits) and incident, prevalent and persistent excess urinary albumin excretion (eUAE) as outcome variables (latter measured at Y20 and/or Y25 examination visits at a mean age of 45 or 50 years)
Discussion
This longitudinal study demonstrates that rapid decline in lung function, although largely within the normal range of lung function, in young to middle-aged healthy adults, predicts incident eUAE excretion later in life. Prevalent eUAE in young adulthood however does not predict rapid decline in lung function later in life in this study. Thus, rapid decline in lung function precedes the development of eUAE, a marker for renovascular and/or cardiovascular endothelial dysfunction.15
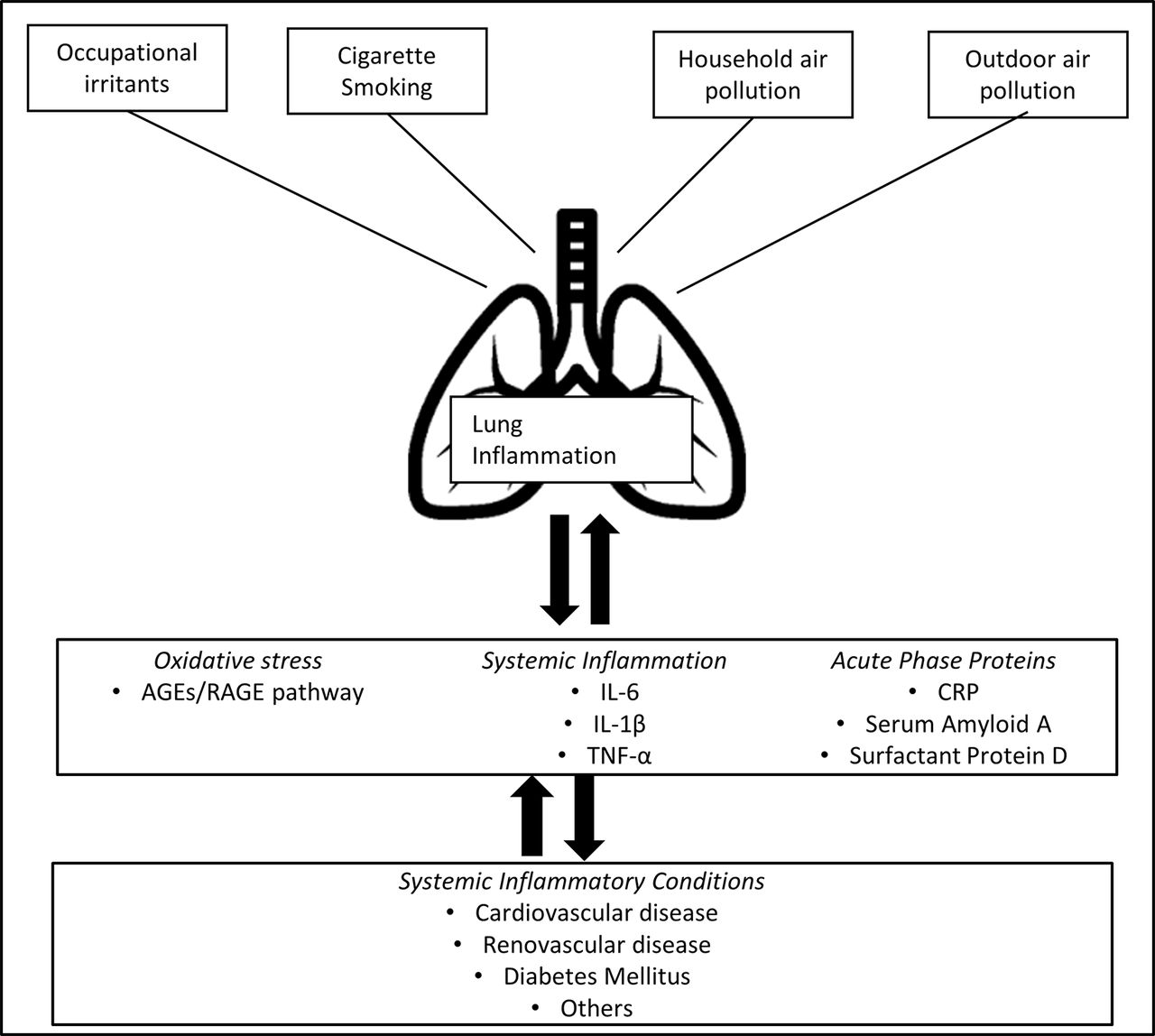
This study used subclinical markers of lung and vascular disease as exposure and outcome variables in healthy adults. Rapid decline in lung function in healthy adults is a subclinical marker for subsequent chronic lung disease.16快速下降的可能机制lead to chronic lung disease include activation of inflammation, elastolytic proteases and oxidative stress, and acceleration of ageing within the lung.17Lung inflammatory markers may spill over into the systemic circulation18and lung oxidative stress may increase advanced glycation end-products (AGEs), activating the ubiquitously expressed transmembrane receptor for AGEs (RAGE), in turn triggering additional inflammation and end organ injury (figure 3).19–21

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Hypothesised conceptual framework of the association between lung and vascular events. Although speculative, the study findings that rapid decline in lung function predicts incident excess urinary albumin excretion later in life may be explained by lung inflammation, which causes a ‘spillover’ of local cytokines, acute-phase proteins and oxidative stress into the systemic circulation. Systemic inflammation in turn may affect endothelial function in renovascular and cerebrovascular beds, leading to renovascular and cardiovascular diseases. Alternatively, vascular endothelial dysfunction and lung inflammation may be two forms of expression of the same systemic inflammatory state, although with differing latency periods. AGEs, advanced glycation end-products; CRP, C reactive protein; IL, interleukin; RAGE, transmembrane receptor for AGEs; TNF-α, tumour necrosis factor-alpha.
Mirroring rapid decline as a subclinical marker for lung disease, eUAE is a subclinical marker for cardiovascular and renovascular diseases, as well as for clinical renal disease.22The MONItoring Trends and Determinants of Cardiovascular Diseases study established that eUAE predicted development of ischaemic heart disease in healthy adults, independently of other traditional risk factors.23Similar findings were noted with respect to cardiovascular mortality in a large study of patients with chronic renal disease.24Miettinenet alfound that the extent of eUAE was cross-sectionally associated with risk for stroke and lower extremity amputation, independently of traditional risk factors.25Not only is eUAE the result of injury to the glomerular filtration barrier by systemic inflammation and oxidant stress but its presence may further promote systemic inflammation and oxidative stress, in turn linking it with adverse vascular outcomes.26
有可能是血管内皮dysfunction results from a systemic ‘spillover’ of the local inflammatory and reparative events occurring in the lungs (figure 3).27Alternatively, vascular endothelial dysfunction and rapid decline may be two forms of expression of the same systemic inflammatory state, although with differing latency periods. Both views have merit but imply different conceptual and therapeutic consequences. In the former, the aim of therapy may be centred in improving lung health and local inflammation, whereas in the latter, the centre of therapy may be shifted to ameliorating the systemic inflammatory state.
Our longitudinal finding that rapid decline in lung function in healthy adults predicts vascular endothelial function is supported by several cross-sectional studies. The third US-based National Health and Nutrition Examination Survey (NHANES III) suggests that low lung function is cross-sectionally associated with eUAE, findings that were also demonstrated by the 5th Korea National Health and Nutrition Examination Survey.28A cross-sectional study of Chinese type 2 diabetics found that gas exchange efficiency during exercise in those with eUAE was lower than those without eUAE.29Additional support for our findings is provided by cross-sectional studies of patients with chronic lung diseases. Casanova's cross-sectional study confirmed that eUAE was more frequent among patients with COPD than healthy smokers (24% vs 6%) and that eUAE was inversely correlated with arterial oxygenation.4Low arterial oxygenation in patients with COPD has in turn been shown by others to be associated with increased risk for death.30Fordet alhave recently demonstrated that the level of UAE is higher in patients with moderate to severe obstructive lung disease compared with those with normal lung function or mild obstructive lung disease. eUAE was also shown to be associated with all-cause mortality among US adults with obstructive lung disease.31最近的一项研究的智慧较小的患者群h COPD confirmed that eUAE was related to the Body mass index, airflow Obstruction, Dyspnea and Exercise capacity (BODE) index. Higher BODE scores have been shown to predict mortality in COPD.32Similarly, there is a limited body of cross-sectional literature that demonstrates that chronic lung disease is associated with atherosclerotic cardiovascular disease, diastolic dysfunction and right and left heart failure.33Also published is the cross-sectional association between chronic lung disease (such as COPD) and kidney disease.34Since we were unable to demonstrate an association between decline in FEV1/FVC ratio and eUAE, our findings may not be COPD specific but may be relevant to chronic lung diseases in general.
Our longitudinal study fills a critical gap in the existing literature by demonstrating the direction of association between lung and vascular outcomes, a key feature that may help establish causality in future studies. Thus, our study clarifies that the low lung function–eUAE relationship is primarily unidirectional—rapid decline in lung function predicts eUAE but not vice versa in healthy adults. Duprezet al35reported in the MESA study that low lung function, although within the normal absolute range, was correlated with small arterial stiffness, a finding confirmed by another NHANES III study as well.36Decline in FVC in the CARDIA cohort has been previously reported to predict diastolic dysfunction.37Jacobset alhave previously reported in the same cohort that decline in lung function in healthy adults predicted future incident systemic hypertension but not vice versa.38Our findings extend this previous understanding by demonstrating that the association between rapid decline and incident eUAE may be similarly unidirectional in healthy adults.
The strengths of our study relate to its longitudinal cohort design, large sample size with repeated measurements, national multicentre patient recruitment, inclusion of a large minority population and women, focus on subclinical outcomes rather than established disease states and a novel hypothesis that could possibly link chronic lung disease to vascular endothelial function. In addition, by excluding the presence of lung and renal disease at the start of the study, our finding of the association between rapid decline and incident eUAE in a healthy population broadens the scope of this association as it has been previously described to be present only in diseased populations. Further, using a relatively young and healthy study population with relatively few comorbidities helps decrease the bias related to the association.
Our study has several limitations. One limitation is that only 117 subjects had eUAE at CARDIA Y10. We may be therefore underpowered to study our second analysis that eUAE predicts rapid decline. Since a small number of subjects with eUAE in our study had severe eUAE (ie, >300 mg/g; consistent with the previously used term macroalbuminuria;online supplementary table E-V), our findings primarily examine moderate eUAE, consistent with the previously used term microalbuminuria. This is acceptable since moderate eUAE or microalbuminuria is an established marker for vascular endothelial function.6While eUAE is a marker for renovascular and/or cardiovascular endothelial dysfunction, there is limited data on its use in predicting outcomes in other vascular beds. Several characteristics of those subjects who were excluded from our study were significantly different from those included, as seen inonline supplementary table E-IV,但这些特点的临床差异stics that do not form the basis for exclusion criteria are quite small. This is therefore an unlikely source for selection bias. In addition, subject-reported physician diagnosis of chronic bronchitis, emphysema or kidney disease at the Y0 visit was used as exclusion criteria instead of standard clinical definitions for these diseases as this information was not available in the CARDIA data set at Y0 visit, which may have resulted in underexclusion or overexclusion of subjects at study start. The study did not exclude subjects with asthma. This approach is reasonable since subjects with asthma do not demonstrate a different rate of FEV1decline than those without asthma.39Additional adjustment for self-reported asthma however did not change the results of the study (seeonline supplementary table E-VI).Exclusion of subjects with missing data may bias results in any cohort study but our high cohort retention rates and non-differential loss to follow-up between those with and without rapid decline indicate that this is an unlikely explanation for our findings. Post-bronchodilator spirometric values were not available. The slope of decline calculated from the post-bronchodilator measurement has however been shown in the literature to have a similar variance as the pre-bronchodilator measurement.40Based on the questionnaire, there were six pregnant women during the Y20 exam and three during the Y25 exam. Additionally, a total of 93 patients in the CARDIA study died of cardiovascular/renovascular causes by the Y25 visit. Patients who died before follow-up were classified as missing data. Since there were very few pregnant women (0.3%) and relatively few deaths (0.5%), they are an unlikely source of misclassification bias. We did not exclude the small number of study participants whose lung function fell outside the normal range; 5.3% of participants at Y5 visit had FEV1below the Hankinson-defined lower limit of normal.41However, lung function below the lower limit of normal at Y5 was not related to rapid decline (p=0.09).
Conclusion
Serial measurement of rapid decline in lung function, but still largely within the normal range of absolute lung function, in young to mid adulthood, can be used in healthy individuals to predict future risk for renovascular and cardiovascular endothelial dysfunction, as assessed by incident eUAE. The implication of our study findings is that improvement in lung health and in lung and/or systemic inflammation may help improve vascular endothelial function, thereby decreasing the morbidity and mortality related to renovascular and cardiovascular diseases.
Unadjusted association between prevalent excess urinary albumin excretion (eUAE) at Coronary Artery Risk Development in Young Adults (CARDIA) Y10 visit as the predictor variable and rapid lung function decline as outcome variable (latter measured between CARDIA Y10 and Y20 visits)
Acknowledgments
The authors thank Dr William Beckett, Mount Auburn Hospital, Cambridge, MA, USA, and Dr Mark Unruh, University of New Mexico School of Medicine, Albuquerque, NM, USA, for their reviews of the manuscript.
References
Footnotes
ContributorsSB, TAC, HK, DD, BC, AS, BT, RK, LJS and DRJ made substantial contributions to the conception or design of the work and CQ and AA made substantial contributions to the acquisition, analysis or interpretation of data for the work. SB, TAC, HK, DD, BC, AS, BT, RK, LJS, DRJ, CQ and AA made substantial contribution towards drafting the work or revising it critically for important intellectual content. SB, TAC, HK, DD, BC, AS, BT, RK, LJS, DRJ, CQ and AA provided the final approval of the version to be published, agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
FundingThe Coronary Artery Risk Development in Young Adults Study (CARDIA) is conducted and supported by the National Heart, Lung, and Blood Institute (NHLBI) in collaboration with the University of Alabama at Birmingham (HHSN268201300025C and HHSN268201300026C), Northwestern University (HHSN268201300027C), University of Minnesota (HHSN268201300028C), Kaiser Foundation Research Institute (HHSN268201300029C) and Johns Hopkins University School of Medicine (HHSN268200900041C). CARDIA is also partially supported by the Intramural Research Program of the National Institute on Aging (NIA) and an intraEagency agreement between NIA and NHLBI (AG0005). This manuscript has been reviewed by CARDIA for scientific content.
Competing interestsNone declared.
Patient consentObtained.
Ethics approvalIRB approval was obtained by the CARDIA study and all individual study sites.
Provenance and peer reviewNot commissioned; externally peer reviewed.
Data sharing statementCARDIA study allows for data sharing with approval with other investigators.